
The clinical assessment of coronary artery calcium (CAC) has undergone a paradigm shift over the past three decades, evolving from a research tool to a central instrument in cardiovascular risk stratification. Central to this transformation is the concept of the coronary artery calcium score of zero—commonly referred to as the “power of zero”—which has emerged as one of the most powerful negative risk markers in preventive cardiology [1]. In appropriately selected populations, a CAC score of zero confers substantial short- and intermediate-term prognostic reassurance. However, the interpretation of CAC = 0 is not uniform across clinical contexts. Residual risk diverges significantly between asymptomatic individuals undergoing primary prevention screening and symptomatic patients presenting with chest pain.
The presence of coronary calcium represents a biologic response to chronic lipid infiltration and inflammation within the arterial intima [2]. Calcification reflects advanced atherosclerotic remodeling involving osteogenic differentiation and extracellular matrix changes. However, calcification detectable on non-contrast CT captures only macroscopic mineralization and does not quantify non-calcified plaque components, including lipid-rich necrotic cores and fibrous tissue [3]. Thus, absence of calcium does not equate to absence of atherosclerosis.
Biological Foundations of Coronary Calcification
CAC scoring is performed using non-contrast, ECG-gated CT imaging. The Agatston score multiplies plaque area by a density weighting factor derived from peak attenuation ≥130 Hounsfield Units (HU) [2]. Lesions below this threshold are not considered calcified.
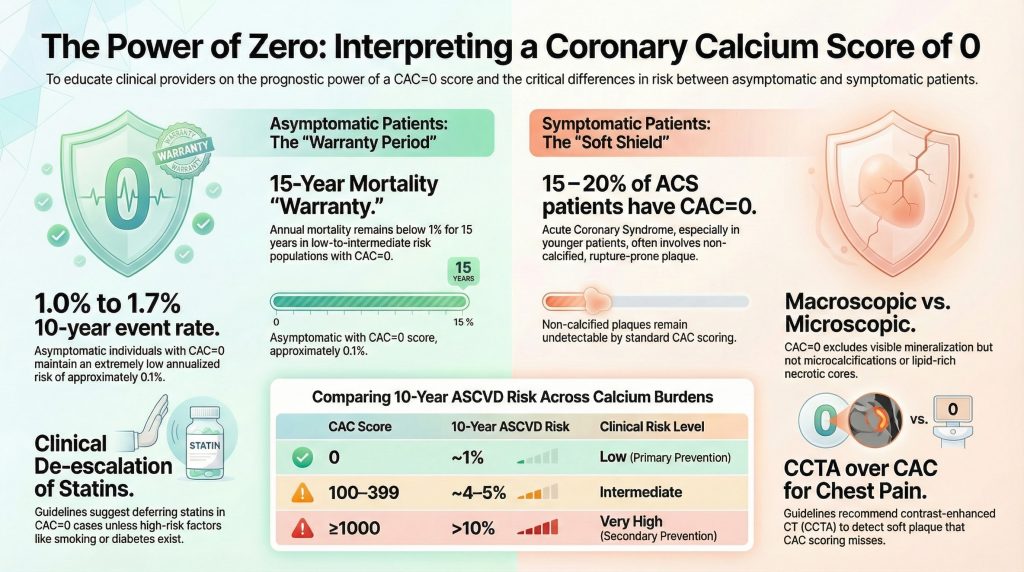
In contrast-enhanced coronary CT angiography (CCTA), plaque characterization differentiates necrotic core, fibrofatty, fibrous, and calcified components based on attenuation ranges [3]. Importantly, rupture-prone plaques frequently contain large necrotic cores with thin fibrous caps and minimal macrocalcification [4].
A critical mechanistic distinction exists between macrocalcification and microcalcification. Dense macrocalcification visible on CT often reflects plaque stabilization and healing. In contrast, microscopic calcifications—below CT resolution—can generate mechanical stress within the fibrous cap and increase rupture susceptibility [5]. Therefore, CAC = 0 excludes macroscopic calcification but does not exclude microcalcific activity or vulnerable plaque biology.
The Asymptomatic Population: The Power of Zero
In the Multi-Ethnic Study of Atherosclerosis (MESA), approximately 50% of middle-aged asymptomatic adults demonstrated CAC = 0 at baseline [6]. Long-term follow-up revealed 10-year ASCVD event rates of approximately 1–1.7% among these individuals, corresponding to an annualized risk near 0.1% [6,7]. These event rates are substantially lower than predicted by traditional risk models in many intermediate-risk individuals.
Even minimal calcification (CAC 1–10) confers approximately a threefold increase in coronary heart disease risk compared with CAC = 0 [6]. Thus, CAC = 0 represents a biologically distinct low-risk phenotype rather than merely the lowest point on a continuum.
Graded Risk Across CAC Categories
Risk increases stepwise with rising calcium burden [7,8]:
- CAC = 0: ~1% 10-year risk
- CAC 1–99: ~1.9% 10-year risk
- CAC 100–399: ~4–5% 10-year risk
- CAC ≥400: ~7–9% 10-year risk
- CAC ≥1000: >10%, approaching secondary-prevention populations
Individuals with CAC ≥1000 exhibit cardiovascular mortality rates comparable to stable secondary-prevention cohorts, including those similar to FOURIER trial participants [8]. This observation supports aggressive lipid-lowering strategies in extreme CAC categories.
NNT Modeling and Therapeutic Allocation
CAC scoring refines statin allocation efficiency. Among intermediate-risk individuals:
- CAC = 0: 5-year Number Needed to Treat (NNT) often exceeds 100
• CAC >100: 5-year NNT often ranges between 12–25 [1,9]
Most absolute statin benefit accrues to patients with measurable calcified burden. The 2018 ACC/AHA cholesterol guidelines recommend that statin therapy may be deferred in asymptomatic individuals with CAC = 0 unless diabetes, smoking, or strong family history is present [9].
Soft Plaque and “Warranty” Periods
The Miami Heart Study demonstrated that approximately 16% of asymptomatic individuals with CAC = 0 have non-calcified plaque on CCTA [10]. However, obstructive stenosis (≥50%) was present in only 0.8%, and high-risk plaque features were uncommon. Thus, while soft plaque is detectable, it rarely reaches clinical significance in asymptomatic zero-CAC individuals.
A prospective study of 9,715 asymptomatic individuals demonstrated that CAC = 0 confers a 15-year mortality “warranty period” in low-to-intermediate risk populations [11]. Annual mortality remained below 1% during this interval. However, this warranty is shortened in diabetics and heavy smokers due to accelerated plaque progression [12].
Sex-Specific Nuance and Ethnic Variability
Women generally exhibit lower absolute CAC prevalence compared with men but may harbor a greater proportion of non-calcified plaque [13]. Consequently, while CAC = 0 remains prognostically powerful in women, symptomatic female patients may require more cautious interpretation. Women presenting with chest pain frequently demonstrate non-obstructive CAD or microvascular dysfunction, conditions not reliably captured by CAC scoring alone.
MESA demonstrated significant ethnic heterogeneity in CAC prevalence [6]. White individuals exhibit the highest CAC prevalence, followed by Hispanic, Black, and Chinese American populations. Despite differences in prevalence, event rates at comparable CAC levels are similar across ethnic groups, reinforcing that CAC = 0 confers prognostic reassurance across diverse populations.
The Symptomatic Population: Residual Risk
In patients presenting with stable chest pain, CAC = 0 does not exclude coronary disease. Approximately 7–16% demonstrate plaque on CCTA, and 1–2% have obstructive CAD ≥50% [14]. In the PROMISE trial, 16.5% of symptomatic zero-CAC patients had non-obstructive CAD, and 1.5% had obstructive disease [15].

Acute Coronary Syndrome and Zero CAC
Pooled analyses demonstrate that 15–20% of patients presenting with acute coronary syndrome (ACS)—particularly younger individuals—may have CAC = 0 at presentation [16]. These findings reflect the predominance of non-calcified, rupture-prone plaque. Accordingly, the 2021 AHA/ACC Chest Pain Guideline recommends CCTA rather than CAC scoring when evaluating possible acute coronary syndrome [17].
Detailed Plaque Morphology: ICONIC Insights
The ICONIC trial quantified plaque components in symptomatic zero-CAC patients who subsequently developed ACS [4]:
- Fibrous plaque: 29.4 mm³ (ACS) vs 5.5 mm³ (controls)
• Fibrofatty plaque: 27.3 mm³ vs 1.3 mm³
• Necrotic-core plaque: 2.8 mm³ vs 0.0 mm³
These quantitative differences confirm that substantial vulnerable plaque burden may exist in the absence of detectable calcification.
Bayesian Interpretation and Risk Modifiers
Diagnostic performance depends on pre-test probability [18]. In asymptomatic individuals with low baseline risk, CAC = 0 reduces post-test probability to near-negligible levels. In symptomatic patients with higher pre-test probability, residual risk remains clinically meaningful despite a zero score.
Additional risk modifiers must be considered. Parental premature cardiovascular disease independently increases risk, even among individuals with CAC = 0 [19]. Furthermore, an elevated Atherogenic Index of Plasma (AIP) correlates with calcification burden and major adverse cardiovascular events independent of traditional risk factors [20].
Conclusion
The coronary artery calcium score of zero is among the most powerful negative risk markers in cardiovascular medicine. In asymptomatic individuals, it confers a prolonged mortality warranty and supports selective de-escalation of pharmacotherapy. In symptomatic patients, however, CAC = 0 represents a “soft shield”—associated with lower risk than positive scores but insufficient to exclude obstructive or vulnerable plaque. Future risk stratification must integrate calcified and non-calcified plaque assessment, clinical phenotype, and individualized risk modifiers rather than relying solely on binary calcium absence.
References
- Hussain A, Ballantyne CM, Nambi V. Zero Coronary Artery Calcium Score: Desirable, but Enough?. Circulation. 2020;142(10):917-919. doi:10.1161/CIRCULATIONAHA.119.045026
- Czaja-Ziółkowska MZ, Wasilewski J, Gąsior M, Głowacki J. An update on the coronary calcium score: a review for clinicians. Postepy Kardiol Interwencyjnej. 2022;18(3):201-205. doi:10.5114/aic.2022.121035
- Vatsa N, Faaborg-Andersen C, Dong T, Blaha MJ, Shaw LJ, Quintana RA. Coronary Atherosclerotic Plaque Burden Assessment by Computed Tomography and Its Clinical Implications. Circ Cardiovasc Imaging. 2024;17(8):e016443. doi:10.1161/CIRCIMAGING.123.016443
- Jonas RA, Nurmohamed NS, Crabtree TR, et al. CTA-Derived Plaque Characteristics and Risk of Acute Coronary Syndrome in Patients With Coronary Artery Calcium Score of Zero: Insights From the ICONIC Trial. AJR Am J Roentgenol. 2025;225(1):e2431476. doi:10.2214/AJR.24.31476
- Hutcheson JD, Goettsch C, Bertazzo S, et al. Genesis and growth of extracellular-vesicle-derived microcalcification in atherosclerotic plaques. Nat Mater. 2016;15(3):335-343. doi:10.1038/nmat4519
- Detrano R, Guerci AD, Carr JJ, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336-1345. doi:10.1056/NEJMoa072100
- Budoff MJ, Shaw LJ, Liu ST, et al. Long-term prognosis associated with coronary calcification: observations from a registry of 25,253 patients. J Am Coll Cardiol. 2007;49(18):1860-1870. doi:10.1016/j.jacc.2006.10.079
- Dzaye O, Razavi AC, Michos ED, et al. Coronary artery calcium scores indicating secondary prevention level risk: Findings from the CAC consortium and FOURIER trial. Atherosclerosis. 2022;347:70-76. doi:10.1016/j.atherosclerosis.2022.02.006
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. doi:10.1161/CIR.0000000000000625
- Nasir K, Cainzos-Achirica M, Valero-Elizondo J, et al. Coronary Atherosclerosis in an Asymptomatic U.S. Population: Miami Heart Study at Baptist Health South Florida. JACC Cardiovasc Imaging. 2022;15(9):1604-1618. doi:10.1016/j.jcmg.2022.03.010
- Valenti V, Ó Hartaigh B, Heo R, et al. A 15-Year Warranty Period for Asymptomatic Individuals Without Coronary Artery Calcium: A Prospective Follow-Up of 9,715 Individuals. JACC Cardiovasc Imaging. 2015;8(8):900-909. doi:10.1016/j.jcmg.2015.01.025
- McClelland RL, Jorgensen NW, Budoff M, et al. 10-Year Coronary Heart Disease Risk Prediction Using Coronary Artery Calcium and Traditional Risk Factors: Derivation in the MESA (Multi-Ethnic Study of Atherosclerosis) With Validation in the HNR (Heinz Nixdorf Recall) Study and the DHS (Dallas Heart Study). J Am Coll Cardiol. 2015;66(15):1643-1653. doi:10.1016/j.jacc.2015.08.035
- Shaw LJ, Raggi P, Callister TQ, Berman DS. Prognostic value of coronary artery calcium screening in asymptomatic smokers and non-smokers. Eur Heart J. 2006;27(8):968-975. doi:10.1093/eurheartj/ehi750
- Wang X, Le EPV, Rajani NK, et al. A zero coronary artery calcium score in patients with stable chest pain is associated with a good prognosis, despite risk of non-calcified plaques. Open Heart. 2019;6(1):e000945. Published 2019 Apr 11. doi:10.1136/openhrt-2018-000945
- Foldyna B, Mayrhofer T, Lu MT, et al. Prognostic value of CT-derived coronary artery disease characteristics varies by ASCVD risk: insights from the PROMISE trial. Eur Radiol. 2023;33(7):4657-4667. doi:10.1007/s00330-023-09430-5
- Gottlieb I, Miller JM, Arbab-Zadeh A, et al. The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography. J Am Coll Cardiol. 2010;55(7):627-634. doi:10.1016/j.jacc.2009.07.072
- Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368-e454. doi:10.1161/CIR.0000000000001029
- Greenland P, Bonow RO, Brundage BH, et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography). Circulation. 2007;115(3):402-426. doi:10.1161/CIRCULATIONAHA..107.181425
- Lloyd-Jones DM, Nam BH, D’Agostino RB Sr, et al. Parental cardiovascular disease as a risk factor for cardiovascular disease in middle-aged adults: a prospective study of parents and offspring. JAMA. 2004;291(18):2204-2211. doi:10.1001/jama.291.18.2204
- Yao H, Feng G, Liu Y, Chen Y, Shao C, Wang Z. Coronary artery calcification burden, atherogenic index of plasma, and risk of adverse cardiovascular events in the general population: evidence from a mediation analysis. Lipids Health Dis. 2024;23(1):258. Published 2024 Aug 20. doi:10.1186/s12944-024-02255-1