
Half of Heart Attacks Have No Warning – Here’s Why
If you woke up tomorrow and saw a strange mole on your skin or felt a painful lump in your neck, you probably wouldn’t ignore it. You would look at it, worry about it, and most likely call a doctor. That reaction is completely natural. As humans, we are wired to respond to things we can see and feel. Visible problems grab our attention and create urgency.
But heart disease doesn’t work like that.
There is no mirror that shows what is happening inside your arteries. There is no visible warning sign, no early pain, no obvious signal that something is wrong. Instead, plaque—the buildup that causes heart attacks—forms slowly and silently over many years. You can feel perfectly fine while the process is already well underway. This creates a dangerous misunderstanding: we assume that if we feel healthy, we are healthy.
This is what can be called a “visibility bias.” We trust what we can see and ignore what we cannot. Unfortunately, when it comes to heart disease, that instinct can lead us in the wrong direction. The most serious threat to your health may be completely invisible.
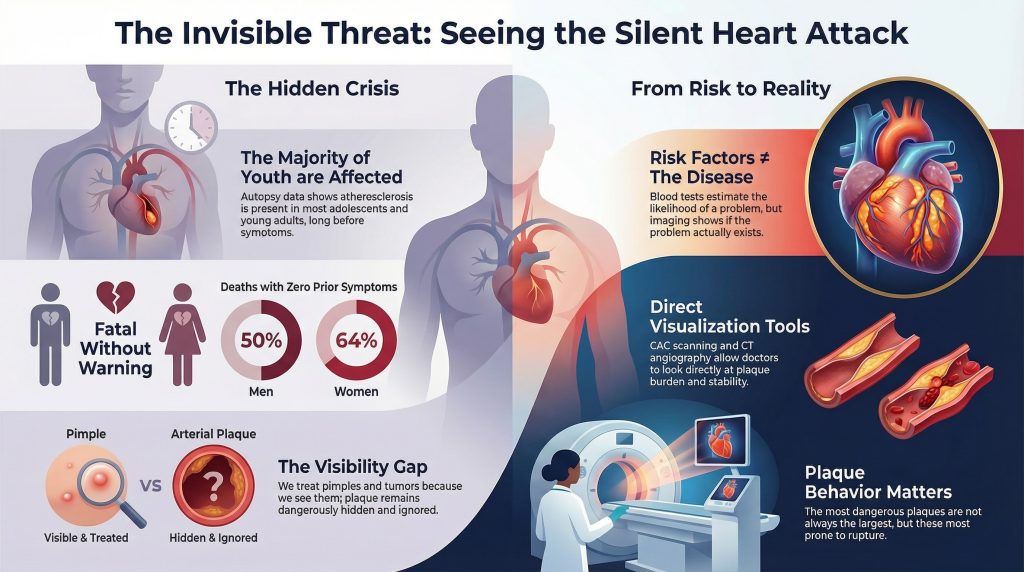
Heart disease is not a sudden event. It is a slow, ongoing process that often begins long before symptoms appear. In fact, research shows that it can start much earlier than most people realize. Many of us think of heart disease as something that happens later in life, perhaps in our 50s or 60s. But studies have shown that plaque buildup, known as atherosclerosis, can begin in childhood or adolescence. The PDAY study, which examined young individuals who died from unrelated causes, found that most already had early signs of artery disease—even though they had no symptoms at all [1].
This finding changes how we should think about heart health. It means that heart disease is not just an “old age” problem. It is a lifelong process that develops quietly over decades. By the time someone reaches middle age, the foundation of the disease may already be in place. Waiting until symptoms appear is like waiting until a small leak turns into a flooded house. The damage is already advanced by the time it becomes obvious.
What makes this even more concerning is how often heart disease gives no warning at all. Many people believe they are safe because they feel good, exercise regularly, or have no chest pain. But the absence of symptoms does not mean the absence of disease. In fact, statistics show that for many people, the first sign of heart disease is a major event like a heart attack or sudden death. According to the American Heart Association, about 50% of men and 64% of women who die from coronary heart disease had no previous symptoms [3]. They felt fine—until they didn’t.
This happens because heart attacks are not always caused by a slow, gradual blockage. Instead, many are triggered by the sudden rupture of a plaque inside the artery. A plaque that was not large enough to cause noticeable problems can suddenly break open, leading to the rapid formation of a blood clot that blocks the artery completely [2]. When that happens, there is no warning period. The event is immediate and often severe.
This challenges another common belief—that heart disease is simply a matter of clogged pipes. Many people imagine arteries like plumbing, where danger only comes from large blockages. But modern research shows that the biology of plaque matters more than its size. Some plaques are stable and may remain harmless for years. Others are unstable, inflamed, and prone to rupture. These unstable plaques are the real danger, and they are not always the biggest ones.
In fact, some of the most dangerous plaques are relatively small. They may not restrict blood flow enough to cause symptoms or show up on a stress test. But if they rupture, they can cause a sudden and catastrophic event. This explains why even people who appear very healthy—including athletes—can sometimes suffer unexpected heart attacks. The issue is not just how much plaque is present, but how active and unstable it is.
For many years, doctors have relied heavily on blood tests, especially cholesterol levels, to estimate heart disease risk. These tests are useful, but they have important limitations. They do not actually show whether plaque is present in the arteries. Instead, they measure conditions that make plaque more likely to form. You can think of it like evaluating the quality of soil without knowing whether anything is actually growing in it.
This means that someone can have high cholesterol but little or no plaque, while another person can have normal cholesterol levels and still have significant buildup. Blood tests provide probabilities, not certainty. They help estimate risk across large groups of people, but they do not always reflect what is happening inside an individual’s body [4].
That is where modern imaging comes in. Today, we have the ability to look directly inside the arteries and see whether plaque is actually present. This is a major shift in how we approach heart disease—from guessing based on risk factors to actually visualizing the disease itself.
One of the most common tools is the coronary artery calcium (CAC) scan. This is a quick, non-invasive test that detects hardened plaque in the arteries and produces a calcium score. This score provides a more direct measure of disease than blood tests alone and can significantly improve risk prediction [5]. Another tool, CT coronary angiography, goes even further by showing both calcified and softer, more dangerous plaques. This allows doctors to see not just how much plaque is present, but also what kind it is.
These imaging technologies act like a “mirror” for your arteries. They allow you and your doctor to see what was once invisible. Instead of relying on indirect clues, you can get a clearer picture of your actual cardiovascular health.
Of course, not everyone needs advanced imaging. But for certain groups of people, it can be especially valuable. This includes those with a family history of heart disease, individuals with borderline or unclear cholesterol levels, people with diabetes or other metabolic conditions, and adults around the age of 40 or older who want a more definitive understanding of their risk. In these cases, imaging can help resolve uncertainty and guide more personalized decisions about prevention and treatment.
There is also a powerful psychological benefit to seeing the disease directly. When people see actual plaque in their arteries, it often makes the risk feel real in a way that numbers on a lab report do not. This can motivate meaningful changes in lifestyle and improve adherence to treatment.
In the end, heart disease remains so dangerous not because we lack knowledge, but because it is so easy to overlook. It develops quietly, without symptoms, and often goes undetected until it is too late. But we now have the tools to change that. We understand that the process begins early, that symptoms are unreliable, and that traditional tests only tell part of the story.
We also have the ability to look directly at the arteries and see what is actually happening.
Heart disease is not a random event. It is a slow, predictable process. The real question is no longer whether it has started—because for many people, it already has.
The real question is whether you choose to look.
References
- McGill HC Jr, McMahan CA, Herderick EE, Malcom GT, Tracy RE, Strong JP. Origin of atherosclerosis in childhood and adolescence. Am J Clin Nutr. 2000 Nov;72(5 Suppl):1307S-1315S.
- Libby P. Mechanisms of acute coronary syndromes and their implications for therapy.
- American Heart Association, “Heart Disease and Stroke Statistics,” 2024.
- Sunkara N, Wong ND, Malik S. Role of coronary artery calcium in cardiovascular risk assessment. Expert Rev Cardiovasc Ther. 2014;12(1):87-94.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol. Circulation.