

The Facts
Are cardiac stents necessary? The short answer: Yes, and no. Although this is a complicated question and the answer can be even more complicated, the most accurate and most straightforward solution is this:
Yes if you are having a heart attack and No, for anything else.
A few facts:
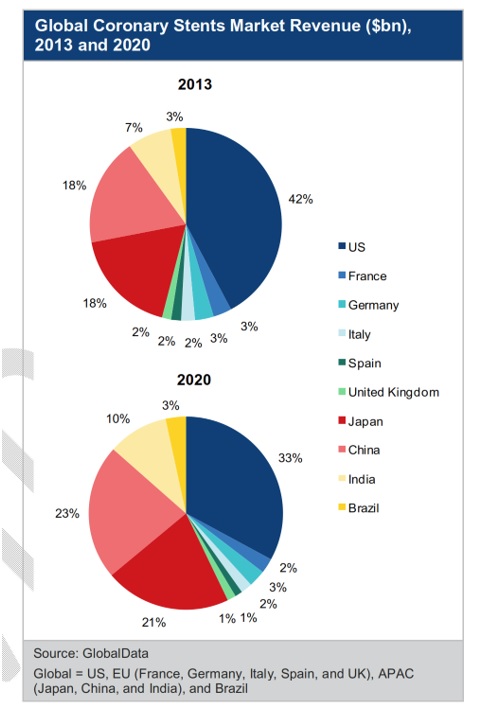
There is a lot of money to be made with cardiac stents by hospitals, cardiologists, drug companies, and of course, medical device manufacturers. (Figure 1) The first bare-metal stents were invented in 1986 and FDA approved in 1992 while in 2003 the first drug-eluting stent was approved.[1, 2] According to iData Research, approximately 1,000,000 stents a year are inserted into coronary arteries in the United States alone.[3](Figure 2) Stents are a $5 billion industry annually, according to GlobalData.[4](Figure 3) Between 2000 and 2006, a world record, as reported by the Guinness Book of World Records, was set with 34 cardiac stents placed in Emil Lohan’s heart. [5][/vc_column_text][vc_column_text]


[/vc_column_text][vc_column_text]
Understanding Cardiac Stents
What are stents anyway?
Stents are tiny metal scaffoldings that are used to force open narrow atherosclerotic arteries. (Figure 4) Many improvements in stent technology have been made over the years. As of 2018, we are on our fourth generation of stents. The metal scaffolding mesh has gotten narrower, which promotes the growth of a monolayer of endothelium (endothelialization) or the ability for the arterial tissue to cover up the metal stent. This is necessary for healthy blood flow in the artery and for preventing blood clots forming in the stent, also called in-stent thrombosis.[6](Figure 5) These new stents are also more flexible to bend into tiny arteries, thereby facilitating placement. The most essential function of the drug is to prevent the stent from becoming clogged with the rapid overgrowth of arterial tissue, also known as neointimal hyperplasia; however, as seen in Figure 5, there is a significant trade-off for this protection with the increase of potentially deadly in-stent thrombosis.[6] This is what happened to my younger brother, who died. Clots can also form in the stent due to incomplete apposition (the stent does not fully deploy or open) leaving a gap that may never endothelialize.


In the mid-80s, physicians used balloon angioplasty to expand the artery without using a stent. A tiny balloon at the end of a catheter was inflated to simply push the plaque out of the way making the artery wider. This technique was less effective, and most arteries soon returned to their previous diameter or worse; therefore stents are now used. Stents cannot be removed.[7] The newest technologies are bioabsorbable (the stent material is eventually degraded and absorbed by the body disappearing over time) and drug impregnated balloon angioplasty. The results of these techniques are approaching that of modern stents but have not yet proved superior.[7] However, their advantage is that no permanent structure is left in the artery. They coat the inside of the artery with an agent similar to the drug-eluting stents. The drug sticks to the artery wall facilitating the patency (openness) of the artery.
Years before the development of drug-eluting stents, bare-metal stents were the only type on the market. The older bare-metal stents had a tendency for generating overgrowth of arterial tissue endothelium (neointimal hyperplasia) around them clogging the artery. [6][7] This occurs most often in smaller arteries and with diabetic patients- which is what happened to my father. The newest drug-eluting stents use much narrower scaffolding and have a polymer coating the metal. The polymer is impregnated with a chemical (usually a chemotherapy agent like paclitaxel or everolimus) that prevent overgrowth of tissue around the stent that can sometimes block the artery. The drug elution usually lasts only a few weeks.
Newest Generation Stents
The newest stents on the market have a dissolvable polymer, so after a few months, the drug goes away, and the polymers coating then resorbs to allow bare- metal underneath the tissue. This is advantageous because the polymer coating on earlier models tended to cause dysfunction in the endothelial tissue surrounding the stent and may cause blood clots to form. It seems that the metal itself does not have the effect of disrupting the endothelial function once the tissue has fully endothelialized. The newest 4th generation stents with dissolvable polymers have a much lower rate of in-stent thrombosis or clotting.
An unforeseen side effect of the drug-eluting stents is that they still have a higher probability of having a clot form in and around the stent.[6](Figure 5) Even though the side-effect of tissue overgrowth has been virtually eliminated, the prospect of in-stent thrombosis is an incessant danger-so, there is some trade-off. Unfortunately, anybody that has a stent must be on antiplatelet therapy for life, usually in the form of aspirin, but dual antiplatelet therapy, which is typically a combination of Clopidogrel and aspirin, is needed to stop clots from forming especially when the stent is new. The most recent guidelines are for about 6 months for dual antiplatelet therapy, but there is increased risk of dangerous bleeding with this therapy (including aspirin monotherapy), so there is some long-term concern for stents from the perspective of anticoagulation therapy.
The Consensus
Evidence has mounted over the years, and the consensus is that there is no advantage for having a stent if a person is currently having an acute coronary syndrome, otherwise known as a heart attack. In 2009 the COURAGE trial determined that there was no advantage to stents vs. optimal medical therapy (using best class drugs). [8]
Following up in 2017, the ORBITA trial was completed, which should have been the nail in the coffin for most stent procedures. ORBITA clearly demonstrated when patients were given a stent or a procedure mimicking stent (sham procedure), there was no evidence of a difference for exercise tolerance or symptoms like chest pain. ORBITA the first placebo-controlled trial ever done! The overarching message is that unless you are having a heart attack, stents show no improvement over medical therapy.
A 2015 update in JAMA (Journal of the American Medical Association) concluded that nearly 80% of all cardiac stents procedures were initially unwarranted according to the current guidelines. [9] Here is a quote from the study authors:
“This systematic review reaffirms the absence of scientific evidence for an initial strategy of PCI[ percutaneous intervention- aka stent] in stable CAD [coronary artery disease]. Despite the evidence, PCI is still commonly used as initial treatment of patients with stable CAD who are asymptomatic or have stable angina and are not on optimal medical therapy. The continued use of PCI for the initial treatment of an obstructive epicardial stenosis reflects persistent adherence to the belief that the epicardial obstruction is the proximate cause of death, myocardial infarction, and angina in stable CAD. However, when the data does not support the existing paradigm, a new paradigm Clinical Review & Education must be formulated to reflect the scientific data and inform practice.”
What Does It All Mean?
Essentially they are saying the medical community is lagging behind the science and physicians just keep stenting patients unnecessarily – AND this is before the ORBITA study came out showing that most of the benefit for stents is from the placebo effect…bottom line, not enough reason to have this dangerous invasive procedure before all other avenues are explored.
Interestingly, no study, to date, has looked at both the combination of whole food plant-based diet combined with optimal medical therapy. Dean Ornish, Satish Gupta, and Caldwell Esselstyn have all revealed remarkable cardiac benefits of low-fat whole food plant based diet alone or in combination with other lifestyle changes lowered angina or chest pain in over 90% of patients, decreased plaque in arteries and reducing heart attacks. [10-12] Work needs to be done on combing these interventions with drug therapy.
This is precisely what I’ve done – combining the best of both worlds – showing a rapid reversal of coronary artery disease and a substantial increase in exercise performance.
- Sigwart, U., et al., Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med, 1987. 316(12): p. 701-6.
- Serruys, P.W., M.J. Kutryk, and A.T. Ong, Coronary-artery stents. N Engl J Med, 2006. 354(5): p. 483-95.
- https://idataresearch.com/over-1-8-million-stents-implanted-per-year-in-the-u-s/.
- https://www.marketresearch.com/product/sample-8538829.pdf.
- http://www.guinnessworldrecords.com/world-records/most-coronary-stent-implants.
- Jakabcin, J., et al., The lack of endothelization after drug-eluting stent implantation as a cause of fatal late stent thrombosis. J Thromb Thrombolysis, 2008. 26(2): p. 154-8.
- Buccheri, D., et al., Understanding and managing in-stent restenosis: a review of clinical data, from pathogenesis to treatment. J Thorac Dis, 2016. 8(10): p. E1150-E1162.
- Maron, D.J., et al., Impact of an initial strategy of medical therapy without percutaneous coronary intervention in high-risk patients from the Clinical Outcomes Utilizing Revascularization and Aggressive DruG Evaluation (COURAGE) trial. Am J Cardiol, 2009. 104(8): p. 1055-62.
- Mitchell, J.D. and D.L. Brown, Update on Percutaneous Coronary Intervention in Stable Coronary Artery Disease. JAMA Intern Med, 2016. 176(12): p. 1855-1856.
- Gupta, S.K., et al., Regression of coronary atherosclerosis through healthy lifestyle in coronary artery disease patients–Mount Abu Open Heart Trial. Indian Heart J, 2011. 63(5): p. 461-9.
- Esselstyn, C.B., Jr., Updating a 12-year experience with arrest and reversal therapy for coronary heart disease (an overdue requiem for palliative cardiology). Am J Cardiol, 1999. 84(3): p. 339-41, A8.
- Ornish, D., et al., Intensive lifestyle changes for reversal of coronary heart disease. JAMA, 1998. 280(23): p. 2001-7.