
Transdermal 17β-Estradiol and Micronized Progesterone in Early Menopause: A More Favorable Cardiovascular Risk Profile Than Oral CEE/MPA, With Limited Hard-Outcome Evidence
Abstract
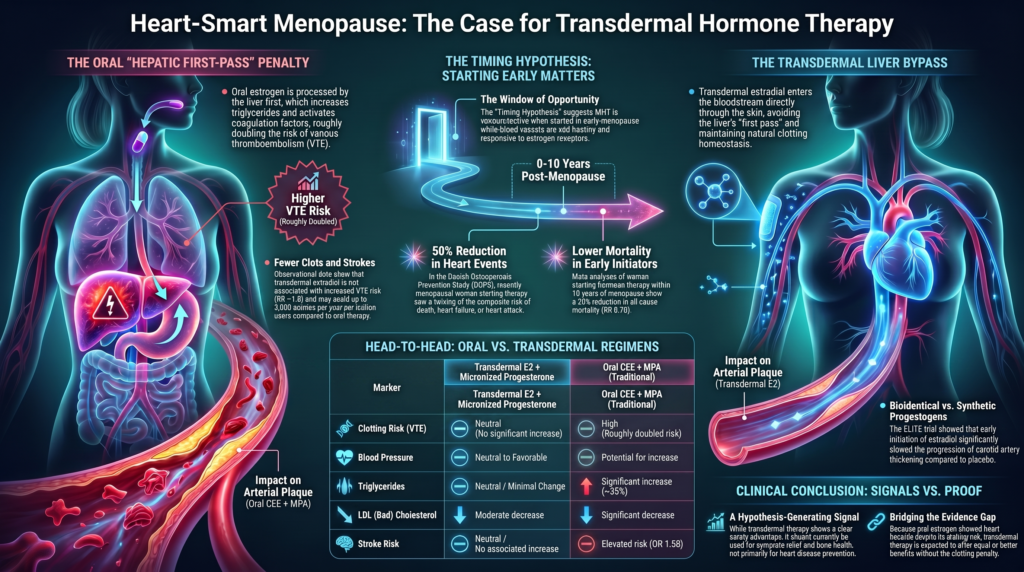
Menopausal hormone therapy’s cardiovascular reputation was shaped by trials of a single oral regimen — conjugated equine estrogens plus medroxyprogesterone acetate (CEE/MPA) — given largely to women a decade or more past menopause. When the lens shifts to early initiation, the signal points the other way. Across a randomized trial (DOPS), the Women’s Health Initiative (WHI) estrogen-alone subgroup of women aged 50–59, meta-analyses of early initiators, and randomized carotid-imaging data (ELITE), hormone therapy begun near menopause is associated with fewer coronary events, less coronary-artery calcium, and lower mortality relative to no therapy. Notably, these benefits were obtained with oral estrogen despite its hepatic, pro-thrombotic liability — the coronary and mortality advantage in early initiators was large enough to coexist with, and in net terms outweigh, the venous-thromboembolism and stroke penalty that the oral route imposes.
Transdermal 17β-estradiol delivers the same bioidentical hormone to the same vascular estrogen receptors, reproducing estrogen’s endothelial, lipid, and anti-inflammatory effects, while bypassing the hepatic first-pass that drives coagulation activation. By extrapolation, transdermal estradiol — paired with metabolically neutral micronized progesterone — may reasonably be expected to retain estrogen’s cardiovascular benefit signal without the clotting penalty that partly offsets it in oral form. Direct hard-endpoint trials of this regimen are lacking not because benefit has been disproven, but because transdermal patches and micronized progesterone are comparatively recent and have not yet been the subject of an adequately powered, long-term cardiovascular-outcomes trial; after WHI, such trials were largely not undertaken. We argue that the convergent early-initiation benefit signal, combined with the mechanistic advantages of the transdermal route, supports transdermal 17β-estradiol with micronized progesterone as the systemic regimen most likely to carry a favorable cardiovascular profile in appropriately selected, recently menopausal women — a strong, testable hypothesis pending confirmatory outcome data, and one that should not be conflated with proven cardiovascular prevention.
Article type. This is a narrative review/commentary, not a primary study or systematic review. It assembles randomized, mechanistic, observational, and guideline evidence; it does not report new human-subjects data, and figures are reproduced from the cited primary publications.
Introduction
The relationship between menopausal hormone therapy (MHT) and cardiovascular disease (CVD) has shifted markedly. Late-twentieth-century observational data suggested cardioprotection; the Women’s Health Initiative (WHI) and the Heart and Estrogen/progestin Replacement Study (HERS) then showed that a specific regimen — oral conjugated equine estrogens (CEE) with the synthetic progestin medroxyprogesterone acetate (MPA) — did not prevent, and in primary prevention modestly increased, coronary and thrombotic events. [1] [2]
Whether those findings should be generalized to modern bioidentical regimens — transdermal 17β-estradiol plus oral micronized progesterone — is the central question here. Review question: does the available randomized, mechanistic, and observational evidence support a more favorable cardiovascular risk profile for transdermal estradiol with micronized progesterone than for the oral CEE/MPA regimen studied in WHI — and, critically, does it support any claim of reduced hard cardiovascular outcomes? We distinguish throughout between hard endpoints (myocardial infarction, stroke, CHD death, major adverse cardiovascular events [MACE]) and surrogate endpoints (lipids, C-reactive protein, endothelial function, carotid intima-media thickness [CIMT], coronary artery calcium [CAC]).
Methods (narrative). Sources were identified through targeted review of randomized trials and their long-term follow-ups, the Cochrane review, major observational cohort/meta-analytic studies of route and progestogen, and major society guidance (ACC/AHA, ESC). Evidence is grouped by endpoint class: randomized hard outcomes, randomized surrogate outcomes, observational thrombosis/stroke outcomes, and mechanistic/metabolic data. This is not a systematic review; no formal search-yield count, risk-of-bias scoring, or meta-analysis was performed. [4]
What the WHI and HERS randomized trials actually showed
WHI randomized 16,608 postmenopausal women with an intact uterus to oral CEE 0.625 mg/day plus MPA 2.5 mg/day or placebo. Over a mean of 5.2 years the regimen increased coronary heart disease (HR 1.29, 95% CI 1.02–1.63), stroke (HR ~1.41), and pulmonary embolism (HR ~2.13), and invasive breast cancer (HR 1.26, 95% CI 1.00–1.59), while reducing hip fracture and colorectal cancer; the global index favored harm (HR ~1.15), and the trial was stopped early. [1]
HERS, a secondary-prevention trial of the same oral CEE/MPA regimen in women with established CHD, found no overall reduction in coronary events and an early excess of events in year one. Together, WHI and HERS justify caution against class-wide extrapolation — but they test one oral regimen and do not establish that an alternative regimen is cardioprotective or even cardiovascular-neutral. [2]
Long-term context matters. In the WHI cumulative 18-year follow-up of 27,347 randomized women, there was no significant difference in all-cause mortality (HR 0.99) or cardiovascular mortality (HR 1.00) between hormone therapy and placebo. The honest reading is therefore neither alarmist nor reassuring about benefit: the regimen carried time-, route-, and formulation-specific nonfatal event risks without a net long-term mortality effect. [3]
Cardiovascular pathophysiology and formulation-specific effects
Route of administration is decisive. Oral estrogen undergoes hepatic first-pass metabolism, raising coagulation factors, sex hormone-binding globulin (SHBG), and renin–angiotensin–aldosterone substrate, and increasing triglycerides; in crossover studies oral estradiol raised large-VLDL apolipoprotein B and triglycerides by roughly 30% and 35%. [14]
Transdermal 17β-estradiol largely bypasses the liver, preserving coagulation homeostasis with minimal triglyceride change and a neutral-to-favorable blood-pressure effect (precise magnitudes vary and are not captured by a single figure). The progestogen matters independently: androgenic synthetic progestins (notably MPA) can blunt estrogen’s vascular and lipid benefits, whereas micronized progesterone is metabolically near-neutral and does not raise blood pressure or LDL. [14] [9] [10]
Directional summary (magnitudes omitted where not traceable to a primary source):
| Marker | Menopause transition | Transdermal E2 + micronized progesterone |
| Blood pressure | Trend toward higher SBP/DBP | Neutral-to-favorable [14] |
| Lipids | ↑ total cholesterol, ↑ LDL | ↓ LDL (less than oral); minimal triglyceride change [14,15] |
| Lipoprotein(a) | Rises across the transition | Lowered, but less than oral estrogen [14,15] |
| Insulin sensitivity | Tendency to insulin resistance | Neutral; no lab-confirmed benefit (KEEPS-Continuation) [8] |
| Heart/visceral fat | ↑ paracardial/visceral fat | Uncertain; see heart-fat analysis [7] |
Hard outcomes versus surrogate markers: a necessary boundary
Favorable changes in LDL-C, triglycerides, CRP, endothelial function, or CIMT are informative but are not equivalent to a proven reduction in MACE. In cardiovascular prevention, event-reduction claims ordinarily rest on large randomized endpoint trials or individual-participant meta-analyses — a standard the promoted MHT regimen has not met for hard outcomes. Much of the mechanistic and surrogate evidence below should be read as supporting plausibility and relative safety, not proof of cardioprotection. [16] [20]
The timing hypothesis and subclinical atherosclerosis (surrogate-level evidence)
The “timing hypothesis” holds that MHT is safer, and possibly vasoprotective, when begun in early menopause when the endothelium still expresses estrogen receptor alpha (ERα) and responds to estradiol via endothelial nitric oxide synthase (eNOS)/nitric oxide (NO) and the G-protein-coupled estrogen receptor (GPER); delayed initiation into aged, plaque-laden vasculature may instead favor pro-inflammatory and matrix-metalloproteinase (MMP)-mediated plaque destabilization. This is a mechanistically grounded hypothesis, supported chiefly by surrogate data. [5]
ELITE randomized 643 women (stratified <6 vs ≥10 years post-menopause) to oral 17β-estradiol 1 mg/day (plus vaginal micronized progesterone gel) or placebo. CIMT progression differed by stratum (P=0.007 for interaction): in the early stratum, 0.0044 mm/yr with estradiol versus 0.0078 mm/yr with placebo (P=0.008), with no benefit in the late stratum. ELITE used oral — not transdermal — estradiol, is a surrogate (CIMT) trial rather than a MACE trial, and its secondary coronary-CT endpoint was null even early; it therefore supports timing-hypothesis vascular findings, not coronary safety of the promoted regimen. [5]
KEEPS compared oral CEE 0.45 mg/day and transdermal E2 50 µg/day (each with cyclic micronized progesterone 200 mg × 12 d/mo) against placebo in 727 women within 3 years of menopause (baseline CAC <50 Agatston units). Over 48 months neither regimen significantly altered CIMT versus placebo; only a non-significant CAC trend favored oral CEE. In a secondary analysis, the paracardial-fat–CAC association was modified by treatment (P=0.02) and significant only in the transdermal arm, while oral CEE was associated with slower epicardial-fat accumulation — reported by the investigators as hypothesis-generating, not as outcome evidence. [6] [7]
The Cochrane review of 19 oral-HT trials (40,410 women) found that initiation <10 years post-menopause was associated with lower all-cause mortality (RR 0.70, 95% CI 0.52–0.95) and lower CHD (RR 0.52, 95% CI 0.29–0.96) but persistent VTE risk (RR 1.74), whereas later initiation conferred no mortality/CHD benefit and increased stroke (RR 1.21, 95% CI 1.06–1.38). These benefit estimates derive from oral HT, so they cannot be transferred directly to transdermal regimens. [4]
Thromboembolic and stroke evidence (largely observational)
Oral estrogen roughly doubles VTE risk (meta-analytic RR ~1.9) via hepatic activation of coagulation; transdermal estradiol is not significantly associated with increased VTE (RR ~1.0), and micronized progesterone is neutral. These comparisons rest mainly on meta-analyses and observational cohorts and are subject to confounding by indication and prescribing selection. [13] [10] [12]
For ischemic stroke, the French E3N-derived case-control analysis found elevated risk with oral estrogen (OR 1.58, 95% CI 1.01–2.49) but not transdermal (OR 0.83, 95% CI 0.56–1.24); micronized progesterone (OR 0.78), pregnanes (OR 1.00), and nortestosterones (OR 1.26) were neutral, whereas norpregnanes were elevated (OR 2.25, 95% CI 1.05–4.81). A Danish national cohort similarly examined stroke by MHT type. The investigators modeled that switching from oral/synthetic to transdermal/micronized regimens could avoid up to ~3,000 strokes per year per million users — a projection, not a trial endpoint, and from observational data. [9] [11]
State of the evidence: what supports a benefit signal — and why it is not proof
It is worth stating plainly where the field actually stands, because “no randomized trial has proven benefit” and “there is no evidence of benefit” are not the same claim. Several lines of evidence, each comparing hormone therapy against no hormone therapy (placebo or no treatment), point in a favorable direction for early initiators — they simply fall short of the standard that would license a prevention claim.
First, the one randomized trial with hard endpoints. The Danish Osteoporosis Prevention Study (DOPS) randomized 1,006 recently menopausal women (mean age ~50) to oral estradiol (with norethisterone acetate in those with a uterus) or no treatment. After ~10 years, the primary composite of death, heart-failure hospitalization, or myocardial infarction occurred in 16 treated versus 33 untreated women — roughly a halving of events — with no excess of breast cancer, venous thromboembolism, or stroke. This is the strongest randomized hard-endpoint signal favoring early initiation relative to no therapy. [25]
Why DOPS is suggestive but not decisive: it was open-label (unblinded), it was designed and powered for fractures rather than cardiovascular events, the event counts were small, and it used oral estradiol/norethisterone — not the transdermal estradiol plus micronized progesterone regimen this review concerns. Notably, in pooled analyses the early-initiation reduction in coronary events reaches significance largely because DOPS is included; restricting meta-analysis to double-blind trials attenuates the effect. DOPS moves the needle toward plausibility; it does not settle the question. [25]
Second, meta-analyses of early initiation versus no therapy. The Cochrane review found that women starting hormone therapy fewer than 10 years after menopause had lower all-cause mortality (RR 0.70) and lower coronary heart disease (RR 0.52) than placebo/no treatment, albeit with persistent venous thromboembolism risk; later initiation showed no such benefit and increased stroke. Independent meta-analyses by Salpeter and colleagues similarly reported lower mortality in trials of younger women and an approximately one-third reduction in coronary events in younger versus older initiators. These analyses pool predominantly oral regimens and are limited by heterogeneity and low event rates. [4] [26] [27]
Third, randomized surrogate and mechanistic data. ELITE showed that, relative to placebo, oral estradiol slowed carotid intima-media thickness progression in women within 6 years of menopause but not in those 10+ years out — a biologically coherent surrogate signal. The endothelial biology (ERα/eNOS/nitric-oxide signaling in healthy vasculature) provides a plausible mechanism. Observational route comparisons consistently favor transdermal estradiol and micronized progesterone for thrombotic and stroke safety relative to oral CEE/synthetic progestins. [5] [9]
Fourth, the WHI’s own early-initiation signals. Although WHI overall showed harm, its pre-specified timing and age analyses point the other way for early initiators. In the pooled WHI timing analysis, the CHD hazard ratio was 0.76 (95% CI 0.50–1.16) for women within 10 years of menopause versus 1.28 (1.03–1.58) at ≥20 years (P for trend = 0.02). In the estrogen-alone trial specifically, women aged 50–59 had a significantly lower composite CHD risk (HR 0.66, 95% CI 0.44–0.97), and in extended follow-up lower myocardial infarction (HR 0.60), CHD (HR 0.65), and total mortality (HR 0.78). The companion coronary-calcium substudy found that women 50–59 randomized to estrogen had less coronary-artery calcium years later (mean score 83.1 vs 123.1), with high-calcium odds roughly 30–40% lower overall and ~60% lower among adherent women — a randomized imaging signal of less atherosclerotic burden. [28] [29]
Positive signals, called out plainly. Pulling these together, the affirmative evidence — all measured against no hormone therapy in early initiators — is the following:
- DOPS: a randomized trial in which early initiation roughly halved the composite of death, heart failure, and MI (16 vs 33 events) with no excess cancer, VTE, or stroke.
- WHI estrogen-alone, ages 50–59: significantly lower CHD (HR 0.66), MI (HR 0.60), and total mortality (HR 0.78), plus less coronary-artery calcium on imaging.
- Cochrane: early initiation associated with lower all-cause mortality (RR 0.70) and CHD (RR 0.52).
- Salpeter meta-analyses: lower mortality in younger-women trials and ~32% fewer coronary events in younger versus older initiators.
- ELITE: slowed carotid atherosclerosis progression with early initiation — a randomized surrogate signal consistent with the above.
One caveat belongs alongside these bullets: in DOPS, cardiovascular events were not the primary endpoint (the trial was designed for fracture prevention) and the absolute event numbers were small, so its hard-outcome signal, while randomized, is hypothesis-strengthening rather than definitive.
What is missing. These signals are convergent and point in the same direction, but each carries a caveat: DOPS was open-label and underpowered and used an oral regimen; the WHI early-initiation findings are subgroup analyses (and the significant CHD reduction is in the estrogen-alone arm); the meta-analytic early-initiation benefit depends partly on the open-label DOPS, attenuating when restricted to double-blind trials; and ELITE/KEEPS measured surrogates, not events (KEEPS was null on CIMT). Above all, there is no adequately powered, blinded, randomized trial of transdermal 17β-estradiol plus micronized progesterone using major adverse cardiovascular events as the primary endpoint. The honest summary is a real, consistent benefit signal for early initiation versus no therapy — strong enough to call out, not strong enough to call proof for the specific modern regimen. [25] [28] [5]
Extrapolating from oral estrogen: the limits of the current trial literature
A central interpretive point follows from the evidence above: almost every positive cardiovascular signal in this field was generated with oral estrogen. That matters in two ways that favor, rather than undercut, the transdermal regimen.
First, oral estrogen produced its early-initiation benefit while carrying a handicap. Oral estrogen roughly doubles venous-thromboembolism risk and raises ischemic-stroke risk through hepatic activation of coagulation. Yet in early initiators the coronary and mortality benefit emerged anyway — the favorable signal in DOPS, the WHI 50–59 subgroup, and the early-initiation meta-analyses was strong enough to coexist with that thrombotic drag. The net cardiovascular result for oral estrogen in younger women was favorable in spite of a built-in clotting penalty, not in the absence of one. [25] [28] [4]
Second, the benefit and the harm arise from separable mechanisms. Estrogen’s vascular benefit is receptor-mediated — activation of ERα/eNOS/nitric-oxide signaling, favorable shifts in LDL and lipoprotein(a), improved endothelial function, and anti-inflammatory effects — and is delivered equally by transdermal 17β-estradiol, which reaches the same systemic receptors. The thrombotic harm, by contrast, is specifically a product of the hepatic first-pass that the oral route imposes and the transdermal route avoids. Removing first-pass delivery therefore removes the principal cardiovascular liability while preserving estrogen’s receptor-mediated vascular effects, and observational route comparisons are consistent: transdermal estradiol with micronized progesterone shows neutral venous-thromboembolism and ischemic-stroke risk while preserving estrogen’s metabolic effects. [9] [10] [13]
The logical extrapolation. If oral estrogen yields a net early-initiation cardiovascular benefit while carrying a thrombotic liability, then transdermal estradiol — preserving estrogen’s receptor-mediated vascular effects without that liability — may reasonably be expected to yield an equal or better net cardiovascular profile. This is the strongest available argument for the modern regimen; it is a mechanistic, bridging argument rather than a direct trial result. [28] [9]
Why the hard-endpoint trials do not yet exist. The absence of definitive outcome evidence for transdermal estradiol plus micronized progesterone reflects limitations in the available trial literature rather than direct evidence against benefit. Transdermal patches and oral micronized progesterone are comparatively recent as the dominant regimen; large cardiovascular-outcomes trials are slow and costly; and after WHI the field largely stopped launching hormone-therapy outcome trials. No adequately powered, blinded trial of this regimen with major adverse cardiovascular events as the primary endpoint has been completed — a gap in what has been studied, not a trial that returned a negative result. [1] [3]
An honest limit on the extrapolation. Bridging is a hypothesis, not an identity. Changing the route changes more than clotting risk: KEEPS suggested transdermal estradiol does not reproduce oral estrogen’s hepatic lipid-lowering potency and, in women with rapid paracardial-fat accumulation, did not slow coronary-artery calcification. So while the transdermal route plausibly preserves most of estrogen’s vascular benefit and sheds its main harm, some portal-dependent effects may not transfer. The extrapolation is strong and testable — it is not proof, and it is the precise question a future outcomes trial should resolve. [6] [7]
Benchmarking against proven LDL-lowering outcome evidence
Because the manuscript discusses estrogen’s lipid effects, it is worth stating plainly what hard-outcome lipid evidence looks like — and that MHT does not meet that bar. In the Cholesterol Treatment Trialists’ meta-analysis (170,000 participants, 26 trials), each 1.0 mmol/L LDL-C reduction lowered major vascular events by ~22% (RR 0.78, 95% CI 0.76–0.80) and all-cause mortality by ~10%, with no threshold; the 2012 low-risk analysis (27 trials, 175,000) showed ~11 fewer major vascular events per 1000 over 5 years per 1.0 mmol/L even at <10% 5-year risk. [16] [17]
Dedicated endpoint trials reinforce this. JUPITER (rosuvastatin in 17,802 adults with low LDL and elevated CRP) was stopped early for benefit; IMPROVE-IT showed that adding ezetimibe to a statin after acute coronary syndrome modestly but significantly reduced events, confirming benefit tracks LDL lowering across drug classes. FOURIER (evolocumab) reduced the primary composite (HR 0.85; 9.8% vs 11.3%), and ODYSSEY OUTCOMES (alirocumab after acute coronary syndrome) reduced the primary endpoint (HR 0.85; 9.5% vs 11.1%) and all-cause death (HR 0.85). [18] [19] [20] [21]
The contrast is the point: unlike statins, ezetimibe, and PCSK9 inhibitors — whose cardiovascular benefits are established in randomized endpoint trials and individual-participant meta-analyses, and which anchor ACC/AHA and ESC prevention guidance — menopausal hormone therapy is not supported by comparably direct evidence for ASCVD event reduction and must not be presented as an evidence-equivalent lipid-lowering or cardioprotective strategy. MHT is indicated for vasomotor symptoms and bone preservation, not for cardiovascular prevention. [22] [23]
Lipids and lipoprotein(a): a clarifying note
Counter-intuitively, the hepatic first-pass that makes oral estrogen less favorable for clotting also makes it a stronger lipid modifier: oral estrogen lowers LDL and Lp(a) more than transdermal estradiol (oral Lp(a) reductions ~22–38% vs transdermal ~8–17% across randomized comparisons), while raising triglycerides; transdermal therapy is triglyceride-neutral. Route selection is thus a trade-off — transdermal optimizes thrombotic/hepatic safety; oral offers stronger Lp(a)/LDL lowering — though no outcome trial has tested Lp(a)-guided route selection. [14] [15]
Clarification regarding cardiovascular disease prevention
Because a common public misconception holds that hormone replacement therapy prevents cardiovascular disease, the position of this review should be unambiguous. Hormone therapy may improve several cardiovascular risk markers and may carry a more favorable risk profile when initiated early after menopause, particularly with transdermal estradiol and micronized progesterone. However, favorable changes in risk factors have not translated into definitive randomized evidence of reduced myocardial infarction, stroke, cardiovascular mortality, or MACE. In summary:
- Hormone therapy can be used for symptom management and bone health.
- Certain formulations (transdermal estradiol with micronized progesterone) appear safer than others (oral CEE with synthetic progestins) from a cardiovascular perspective.
- Hormone therapy should not be prescribed primarily to prevent or treat cardiovascular disease.
- Hormone therapy should not be viewed as evidence-equivalent to proven cardiovascular-prevention therapies such as statins, ezetimibe, or PCSK9 inhibitors.
Guidelines and clinical practice
Consensus guidance (ACC/AHA cholesterol guideline; ESC cardiovascular prevention guideline) centers LDL-C lowering with statins, ezetimibe, and PCSK9 inhibitors for prevention and holds that MHT should not be initiated for primary or secondary cardiovascular prevention; the exact ESC menopause wording should be verified at final reference check. MHT is indicated primarily for the treatment of bothersome vasomotor symptoms and the prevention of menopause-associated bone loss in appropriately selected women. [22] [23]
Pre-initiation risk stratification and preferred regimen
Screen traditional and female-specific risk factors (preeclampsia, gestational diabetes, premature menopause, PCOS); CAC scoring can refine intermediate risk. A markedly elevated CAC burden (e.g., ≥100 AU or ≥75th percentile) warrants individualized caution and generally favors non-hormonal management — framed as relative, not as an absolute contraindication, since no guideline designates a single CAC value as an absolute bar. For symptomatic women within 10 years of menopause at low-to-moderate risk, transdermal 17β-estradiol at the lowest effective dose (typically ≤50 µg/day) with oral micronized progesterone (100 mg/day continuous or 200 mg cyclic × 12 d/mo) is the preferred regimen on safety grounds. [6] [9] [13]
Evidence-strength summary
Endpoint class and access status by source (LDL-lowering trials included only as the external hard-outcome benchmark):
| Study | Formulation / route | Endpoint type | Evidence | Access |
| WHI [1] | Oral CEE+MPA | Randomized hard outcomes | Strong | Full |
| HERS [2] | Oral CEE+MPA (2° prev.) | Randomized hard outcomes | Strong | Abstract |
| WHI mortality [3] | Oral CEE±MPA | Randomized, 18-yr mortality | Strong | Abstract-only |
| Cochrane [4] | Oral HT (pooled) | RCT meta-analysis | Moderate | Full |
| ELITE [5] | Oral E2 + vaginal P4 | Randomized surrogate (CIMT) | Moderate | Full |
| DOPS [25] | Oral E2 ± NETA vs none | Randomized hard composite (open-label) | Moderate (signal) | Full |
| WHI E-alone 50–59 [28,29] | Oral CEE vs placebo | RCT subgroup + CAC imaging | Moderate (signal) | Abstract/Full |
| KEEPS [6,7] | Oral CEE / transdermal E2 | Randomized surrogate (CIMT/CAC) | Moderate | Abstract/Full |
| Canonico/Løkkegaard [9,11] | Oral vs transdermal | Observational stroke/VTE | Low–moderate | Full/Abstract |
| CTT, FOURIER, ODYSSEY [16,17,20,21] | Statin/PCSK9 (LDL benchmark) | Randomized hard outcomes | Strong (benchmark only) | Abstract/Full |
Conclusions
The positive cardiovascular signals deserve to be stated plainly. Compared with no hormone therapy, early initiation has been associated with meaningful benefit across several lines of evidence: a randomized trial (DOPS) in which the composite of death, heart failure, and myocardial infarction was roughly halved; the WHI estrogen-alone subgroup of women aged 50–59, with significantly lower CHD (HR 0.66), myocardial infarction (HR 0.60), and total mortality (HR 0.78) and less coronary-artery calcium on imaging; meta-analytic reductions in all-cause mortality (RR 0.70) and CHD (RR 0.52) for early initiators; an approximately one-third reduction in coronary events in younger women in the Salpeter analyses; and slowed carotid atherosclerosis in ELITE. These signals are consistent in direction and concentrated, as the timing hypothesis predicts, in women who begin therapy near menopause. [25] [28] [29] [4] [5]
On formulation, transdermal 17β-estradiol with oral micronized progesterone has a more favorable thromboembolic, stroke, and metabolic profile than oral CEE/MPA, so it is the regimen best positioned to carry these early-initiation benefits with the least offsetting risk. Because the positive signals were obtained with oral estrogen despite its clotting liability, and because that liability is a route-specific (hepatic first-pass) phenomenon that the transdermal route avoids while preserving estrogen’s receptor-mediated vascular benefit, it is reasonable to extrapolate that transdermal estradiol should retain the benefit signal without the offsetting harm. The lack of a hard-endpoint trial for this regimen reflects its comparative newness and the post-WHI halt in hormone-therapy outcomes trials — a limitation of the available trial literature rather than direct evidence against benefit. [9] [13] [28]
These are signals, not proof. The hard-endpoint trial (DOPS) was open-label and underpowered and used an oral regimen; the WHI benefits are subgroup findings; the pooled early-initiation benefit depends partly on the open-label DOPS; and ELITE/KEEPS measured surrogates rather than events. No adequately powered, blinded, randomized MACE trial of transdermal estradiol plus micronized progesterone exists, and the early-initiation mortality/CHD evidence derives largely from oral regimens. [25] [28] [5]
The defensible conclusion is therefore a calibrated one: among systemic hormone therapy options, transdermal estradiol with micronized progesterone is generally considered a preferred regimen on thrombotic and metabolic safety grounds for appropriately selected symptomatic women in early menopause, and the available evidence — while not definitive — points toward a favorable cardiovascular profile relative to no therapy when initiated early. It remains, however, an option for symptom relief and bone health rather than a cardiovascular-prevention therapy, and it is not evidence-equivalent to proven LDL-lowering treatment. [1] [3] [22]
References
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. 2002;288(3):321-333. doi:10.1001/jama.288.3.321 [Full]
- Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin Replacement Study (HERS) Research Group. JAMA. 1998;280(7):605-613. doi:10.1001/jama.280.7.605 [Abstract]
- Manson JE, Aragaki AK, Rossouw JE, et al. Menopausal Hormone Therapy and Long-term All-Cause and Cause-Specific Mortality: The Women’s Health Initiative Randomized Trials. JAMA. 2017;318(10):927-938. doi:10.1001/jama.2017.11217 [Abstract-only]
- Boardman HM, Hartley L, Eisinga A, et al. Hormone therapy for preventing cardiovascular disease in post-menopausal women. Cochrane Database Syst Rev. 2015;2015(3):CD002229. Published 2015 Mar 10. doi:10.1002/14651858.CD002229.pub4 [Full]
- Hodis HN, Mack WJ, Henderson VW, et al. Vascular Effects of Early versus Late Postmenopausal Treatment with Estradiol. N Engl J Med. 2016;374(13):1221-1231. doi:10.1056/NEJMoa1505241 [Full]
- Harman SM, Black DM, Naftolin F, et al. Arterial imaging outcomes and cardiovascular risk factors in recently menopausal women: a randomized trial. Ann Intern Med. 2014;161(4):249-260. doi:10.7326/M14-0353 [Abstract]
- El Khoudary SR, Zhao Q, Venugopal V, et al. Effects of Hormone Therapy on Heart Fat and Coronary Artery Calcification Progression: Secondary Analysis From the KEEPS Trial. J Am Heart Assoc. 2019;8(15):e012763. doi:10.1161/JAHA.119.012763 [Full (open access)]
- Kantarci K, Tosakulwong N, Lesnick TG, et al. Cardiometabolic outcomes in Kronos Early Estrogen Prevention Study continuation: 14-year follow-up of a hormone therapy trial. Menopause. 2024;31(1):10-17. doi:10.1097/GME.0000000000002278 [Abstract-only]
- Canonico M, Carcaillon L, Plu-Bureau G, et al. Postmenopausal Hormone Therapy and Risk of Stroke: Impact of the Route of Estrogen Administration and Type of Progestogen. Stroke. 2016;47(7):1734-1741. doi:10.1161/STROKEAHA.116.013052 [Full]
- Canonico M, Oger E, Plu-Bureau G, et al. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation. 2007;115(7):840-845. doi:10.1161/CIRCULATIONAHA.106.642280 [Full]
- Løkkegaard E, Nielsen LH, Keiding N. Risk of Stroke With Various Types of Menopausal Hormone Therapies: A National Cohort Study. Stroke. 2017;48(8):2266-2269. doi:10.1161/STROKEAHA.117.017132 [Abstract (observational)]
- Scarabin PY. Progestogens and venous thromboembolism in menopausal women: an updated oral versus transdermal estrogen meta-analysis. Climacteric. 2018;21(4):341-345. doi:10.1080/13697137.2018.1446931 [Abstract (meta-analysis)]
- Mohammed K, Abu Dabrh AM, Benkhadra K, et al. Oral vs Transdermal Estrogen Therapy and Vascular Events: A Systematic Review and Meta-Analysis. J Clin Endocrinol Metab. 2015;100(11):4012-4020. doi:10.1210/jc.2015-2237 [Abstract]
- Walsh BW, Schiff I, Rosner B, Greenberg L, Ravnikar V, Sacks FM. Effects of postmenopausal estrogen replacement on the concentrations and metabolism of plasma lipoproteins. N Engl J Med. 1991;325(17):1196-1204. doi:10.1056/NEJM199110243251702 [Full]
- Hemelaar M, van der Mooren MJ, Mijatovic V, et al. Oral, more than transdermal, estrogen therapy improves lipids and lipoprotein(a) in postmenopausal women: a randomized, placebo-controlled study. Menopause. 2003;10(6):550-558. doi:10.1097/01.GME.0000064866.58809.E5 [Abstract]
- Cholesterol Treatment Trialists’ (CTT) Collaboration, Baigent C, Blackwell L, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376(9753):1670-1681. doi:10.1016/S0140-6736(10)61350-5 [Abstract]
- Cholesterol Treatment Trialists’ (CTT) Collaborators, Mihaylova B, Emberson J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet. 2012;380(9841):581-590. doi:10.1016/S0140-6736(12)60367-5 [Abstract]
- Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008;359(21):2195-2207. doi:10.1056/NEJMoa0807646 [Abstract]
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N Engl J Med. 2015;372(25):2387-2397. doi:10.1056/NEJMoa1410489 [Abstract]
- Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017;376(18):1713-1722. doi:10.1056/NEJMoa1615664 [Full]
- Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N Engl J Med. 2018;379(22):2097-2107. doi:10.1056/NEJMoa1801174 [Full]
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2019;73(24):3168-3209. doi:10.1016/j.jacc.2018.11.002 [Full]
- V Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021;42(34):3227-3337. doi:10.1093/eurheartj/ehab484 [Full]
- Newman CB, Preiss D, Tobert JA, et al. Statin Safety and Associated Adverse Events: A Scientific Statement From the American Heart Association. Arterioscler Thromb Vasc Biol. 2019;39(2):e38-e81. doi:10.1161/ATV.0000000000000073 [Full]
- Schierbeck LL, Rejnmark L, Tofteng CL, et al. Effect of hormone replacement therapy on cardiovascular events in recently postmenopausal women: randomised trial. BMJ. 2012;345:e6409. Published 2012 Oct 9. doi:10.1136/bmj.e6409 [Full]
- Salpeter SR, Walsh JM, Greyber E, Ormiston TM, Salpeter EE. Mortality associated with hormone replacement therapy in younger and older women: a meta-analysis. J Gen Intern Med. 2004;19(7):791-804. doi:10.1111/j.1525-1497.2004.30281.x [Abstract]
- Salpeter SR, Walsh JM, Greyber E, Salpeter EE. Brief report: Coronary heart disease events associated with hormone therapy in younger and older women. A meta-analysis. J Gen Intern Med. 2006;21(4):363-366. doi:10.1111/j.1525-1497.2006.00389.x [Abstract]
- Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA. 2007;297(13):1465-1477. doi:10.1001/jama.297.13.1465 [Abstract]
- Manson JE, Allison MA, Rossouw JE, et al. Estrogen therapy and coronary-artery calcification. N Engl J Med. 2007;356(25):2591-2602. doi:10.1056/NEJMoa071513 [Full]
Access key: “Full” = full text reviewed; “Abstract” / “Abstract-only” = abstract/indexed record reviewed (paywalled full text); “metadata verified” = title/journal/identifiers confirmed via indexing where the abstract was not directly retrievable. Volume/page details, ESC menopause wording, and the Hemelaar pagination should receive a final proof-stage check against the journal of record. An optional mechanistic JCI citation (Kesaniemi & Grundy, J Clin Invest 1982) was suggested in review and may be added if a JCI-level LDL-biology background is desired — confirm details before inclusion.