
Executive Summary: The Paradigm Shift in Acute Coronary Syndromes
For much of modern cardiology, acute myocardial infarction (AMI) has been dominated by a “plumbing model”: atherosclerotic plaque accumulates over years, progressively narrows the coronary lumen, and ultimately ruptures, triggering thrombosis and an abrupt, flow-limiting occlusion. This paradigm remains central to the majority of myocardial infarctions. However, contemporary cardiovascular science has forced a major refinement: a true myocardial infarction can occur even when coronary angiography shows no obstructive stenosis. This clinical entity—myocardial infarction with non-obstructive coronary arteries (MINOCA)—is no longer regarded as an anomaly or exclusionary curiosity, but rather as a heterogeneous ischemic syndrome that requires structured evaluation and mechanism-directed therapy.¹
This report verifies the key mechanisms, definitions, and landmark evidence supporting modern MINOCA care, with particular focus on the 2019 American Heart Association (AHA) Scientific Statement¹ and the Women’s Heart Attack Research Program (HARP) multimodality imaging study.² The core evidence supports several conclusions with high confidence:
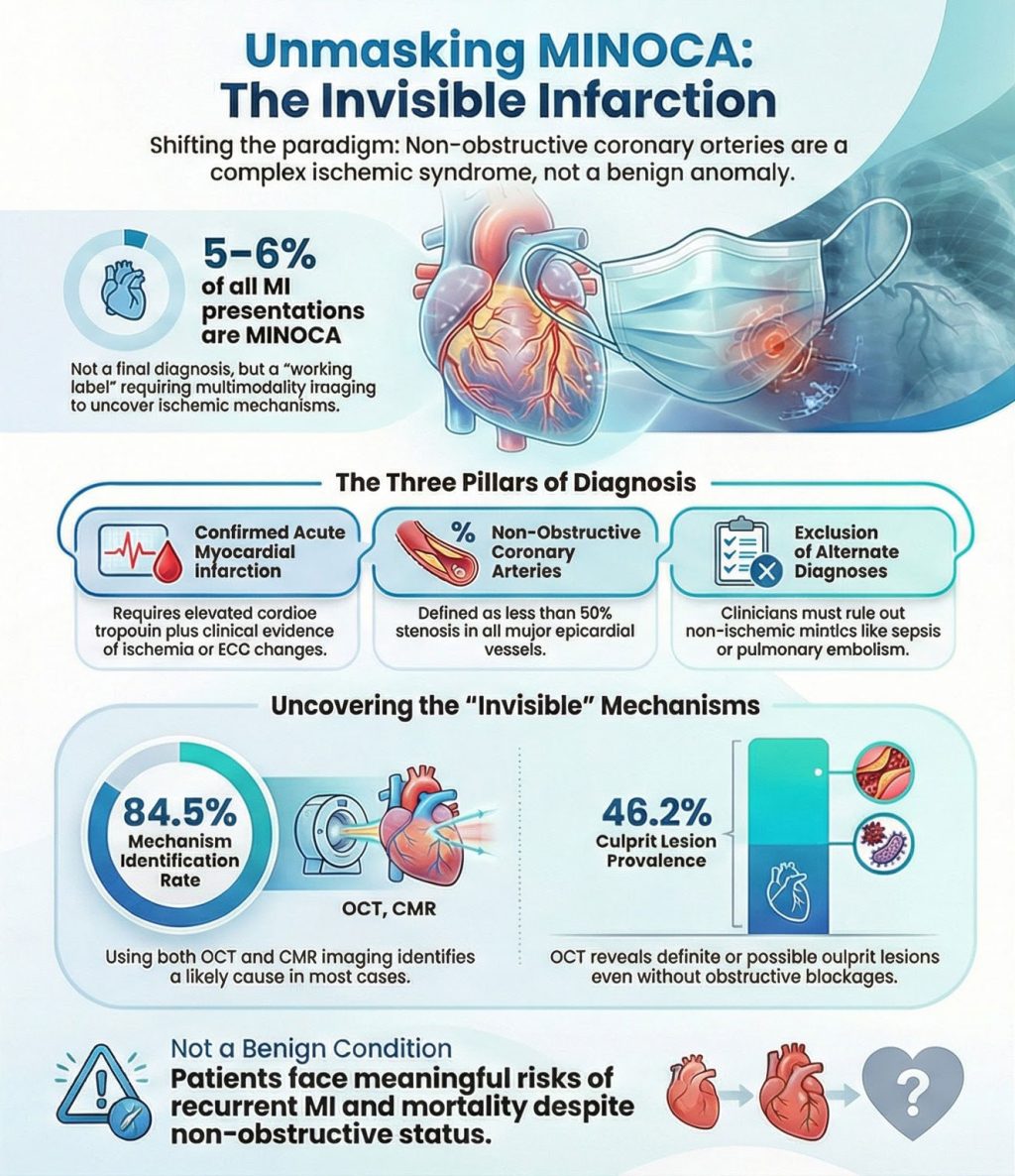
- MINOCA is not rare and accounts for approximately 5–6% of MI presentations, with reported ranges varying by population and operational definition¹,⁴;
- MINOCA is explicitly framed as a working diagnosis, not a final label¹;
- Intravascular imaging (optical coherence tomography, OCT) and cardiac magnetic resonance (CMR) identify a likely mechanism in a high proportion of women with MINOCA (≈84.5% among those undergoing both modalities in HARP)²; and
- the frequently cited “46%” statistic from HARP refers to OCT-identified definite or possible culprit lesions, not “46% plaque rupture.”²


Chapter 1: Historical Context and the Modern Definition
1.1 From diagnostic dismissal to structured clinical framework
Historically, patients—particularly women—presenting with chest pain, biomarker elevation, and non-obstructive coronary angiography were variably labeled with ambiguous or dismissive terms. This contributed to under-recognition, inconsistent management, and inadequate secondary prevention. Contemporary consensus has reversed this approach: MINOCA is now recognized as a genuine MI phenotype encompassing multiple ischemic mechanisms and several clinically important non-ischemic mimics.
The most influential U.S. consensus document is the 2019 AHA Scientific Statement chaired by Tamis-Holland, which formalized a practical definition of MINOCA and emphasized its use as a working diagnosis requiring further investigation rather than a diagnostic endpoint.¹
1.2 The three diagnostic pillars (AHA + Universal Definition alignment)
The AHA statement explicitly aligns MINOCA with the Fourth Universal Definition of Myocardial Infarction.¹,³ Diagnosis requires fulfillment of three pillars:
Pillar 1: A true acute myocardial infarction.
This requires detection of a rise and/or fall in cardiac troponin with at least one value above the 99th percentile upper reference limit, plus evidence of myocardial ischemia, including ischemic symptoms, new ischemic ECG changes, pathological Q waves, imaging evidence of new ischemic myocardial injury, or identification of coronary thrombus.¹,³ The Universal Definition underscores the critical distinction between myocardial injury (non-ischemic mechanisms) and myocardial infarction (ischemic mechanisms).³
Pillar 2: Non-obstructive epicardial coronary arteries.
Non-obstructive disease is pragmatically defined as no coronary stenosis ≥50% in any major epicardial vessel on angiography.¹ The statement acknowledges the limitations of visual angiographic estimation and notes that physiologic assessment (e.g., fractional flow reserve) may be considered in selected cases, but the ≥50% angiographic threshold remains the operational definition.¹
Pillar 3: No alternate diagnosis explaining the presentation.
MINOCA is a label applied after angiography but before exclusion of non-ischemic mimics or systemic causes of troponin elevation. The AHA statement emphasizes ruling out overt alternative diagnoses (e.g., sepsis, pulmonary embolism) and recognizing subtler mimics such as myocarditis or takotsubo syndrome that can resemble MI at presentation.¹,³
Chapter 2: Epidemiology, Demographics, and Why Definitions Matter
2.1 General prevalence and variability
MINOCA prevalence varies substantially depending on cohort selection and diagnostic rigor. The AHA Scientific Statement summarizes MINOCA as occurring in approximately 5–6% of MI patients undergoing angiography, while acknowledging broader ranges across studies.¹ A widely cited systematic review by Pasupathy et al. highlights substantial heterogeneity in reported prevalence and outcomes across international cohorts.⁴
2.2 Sex distribution and clinical implications
MINOCA is consistently reported to occur more frequently in women than in men. The AHA statement notes a disproportionate representation of women among MINOCA cases compared with obstructive MI.¹ Large U.S. registry analyses, including the ACTION Registry–Get With The Guidelines, demonstrate that MINOCA is more common among younger patients and women and provide comparative outcome data by sex and obstructive disease status.⁵
2.3 Clarifying misconceptions about “normal arteries”
A persistent misconception is that MINOCA implies “no plaque” or “completely normal coronary arteries.” This is incorrect. MINOCA explicitly includes patients with mild to moderate atherosclerosis, provided no lesion meets the ≥50% stenosis threshold.¹
Importantly, the HARP study does not report a prevalence of “completely normal arteries.” Its primary focus is on imaging-detected mechanisms, not angiographic smoothness rates.² The AHA statement is explicit: MINOCA does not mean normal arteries.¹
Chapter 3: HARP—Unmasking the Invisible With OCT and CMR
3.1 Why HARP was pivotal
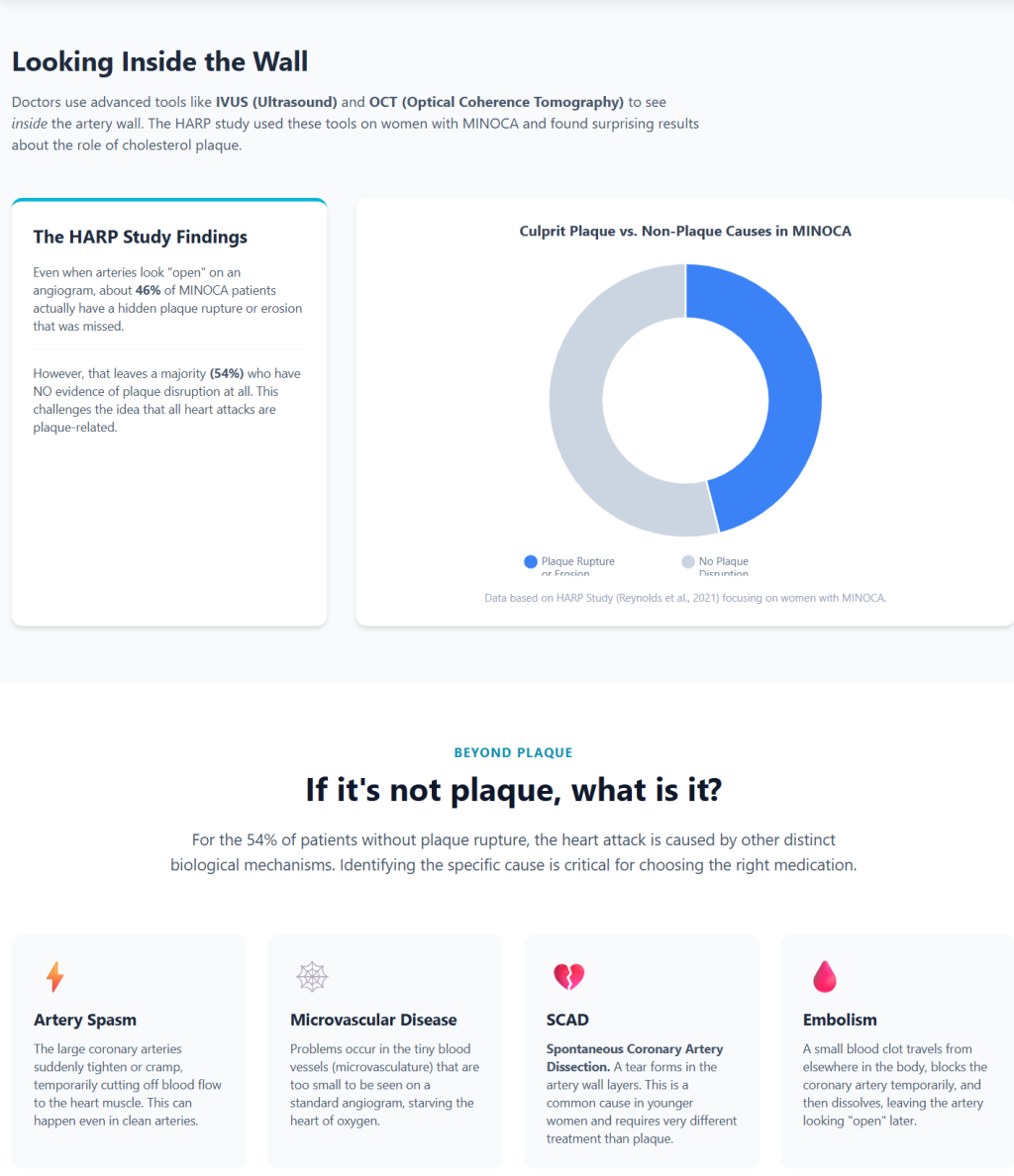
The HARP study fundamentally advanced MINOCA research by applying two complementary imaging modalities: OCT to visualize coronary artery wall pathology and CMR to characterize myocardial injury patterns. This design addressed the central limitation of angiography, which visualizes only the lumen and frequently misses plaque surface disruption, small thrombi, subtle dissections, or transient ischemic mechanisms.²
3.2 Verified enrollment and imaging pipeline
According to the HARP publication:
- 301 women were enrolled across 16 sites
- 170 were diagnosed with MINOCA at angiography
- 145 had OCT images adequate for analysis
- 116 of those underwent CMR
²
3.3 Correct interpretation of the “46.2%” statistic
HARP reports that a definite or possible culprit lesion was identified by OCT in 46.2% (67/145) of participants.² This refers to any OCT-defined culprit lesion, not plaque rupture alone. Treating this number as “46% plaque rupture” is incorrect and unsupported by the primary publication.
3.4 Multimodality diagnostic yield
Among participants who underwent both OCT and CMR, a likely mechanism for the MI presentation was identified in 84.5% (98/116).² This finding strongly supports the AHA’s framing of MINOCA as a diagnosis that benefits from layered evaluation rather than diagnostic closure.¹,²
Chapter 4: Mechanisms of the “Invisible” Infarction
MINOCA is a phenotype encompassing multiple ischemic mechanisms, as outlined in the AHA Scientific Statement.¹
4.1 Plaque disruption without obstructive stenosis
Plaque rupture or erosion can occur in lesions that never produced ≥50% stenosis. Resulting thrombus may be transient, partially lysed, or embolize distally, leaving a non-obstructive angiogram despite true ischemic injury. The AHA statement highlights plaque disruption as a common mechanism and supports intracoronary imaging when appropriate.¹ Classic IVUS studies provide conceptual support for this mechanism.⁶
4.2 Coronary vasospasm
Intense, transient vasoconstriction of an epicardial artery can produce ischemia and infarction, then resolve before angiography. The AHA statement discusses vasospasm mechanisms and the selective use of provocative testing.¹
4.3 Coronary microvascular dysfunction
Microvascular dysfunction involves impaired regulation of small intramyocardial vessels not visualized on angiography. The AHA statement acknowledges CMD as a potential mechanism and emphasizes uncertainty in determining causality versus consequence in individual patients.¹,³
4.4 Coronary embolism or thrombosis
Embolic or thrombotic events can cause transient obstruction or distal microvascular occlusion with minimal residual epicardial disease. The AHA statement outlines selective evaluation, including thrombophilia testing when appropriate.¹
4.5 Spontaneous coronary artery dissection (SCAD)
SCAD is a critical non-atherosclerotic cause of MI, particularly in younger and middle-aged women. Angiographic appearances may be subtle, and intracoronary imaging can be required in selected cases. The AHA SCAD Scientific Statement provides authoritative guidance, and the MINOCA statement emphasizes careful angiographic review for overlooked SCAD.¹,⁷
Chapter 5: Prognosis—Dispelling the “Benign” Myth
MINOCA is not benign. Although outcomes may be better than in extensive obstructive CAD, patients face meaningful risks of recurrent symptoms, recurrent MI, and mortality.¹ Registry analyses, including ACTION Registry–GWTG studies, provide comparative outcome data and reinforce the need for structured follow-up.⁵ Contemporary clinical reviews emphasize that inconsistent definitions historically contributed to conflicting prognostic estimates.⁸
Chapter 6: Management—From Uniform Treatment to Cause-Directed Care
Randomized trial evidence is limited because many classic MI trials excluded patients without obstructive CAD. The AHA statement therefore emphasizes mechanism-directed therapy supported by physiology and observational data.¹
The SWEDEHEART registry analysis demonstrated associations between statins and renin–angiotensin system blockers and improved long-term outcomes in MINOCA patients, while routine dual antiplatelet therapy showed no clear overall benefit across the heterogeneous cohort.⁹,¹⁰ These findings are observational and hypothesis-generating, consistent with AHA guidance.¹
Conclusion
MINOCA has evolved from diagnostic confusion to a defined clinical framework. The 2019 AHA Scientific Statement establishes MINOCA as an MI phenotype requiring exclusion of mimics and pursuit of a specific ischemic mechanism.¹ The HARP study demonstrates that when OCT and CMR are applied, a likely mechanism can be identified in the majority of women studied (≈84.5%), and that nearly half have an OCT-defined culprit lesion despite non-obstructive angiography.²
The core implication is clear: **a non-obstructive angiogram is not a dismissal—it is an invitation to look deeper.**¹,²,³
References
- Tamis-Holland JE, Jneid H, Reynolds HR, et al. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation. 2019;139(18):e891-e908. doi:10.1161/CIR.0000000000000670
- Reynolds HR, Maehara A, Kwong RY, et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women. Circulation. 2021;143(7):624-640. doi:10.1161/CIRCULATIONAHA.120.052008
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. doi:10.1093/eurheartj/ehy462
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131(10):861-870. doi:10.1161/CIRCULATIONAHA.114.011201
- Smilowitz NR, Mahajan AM, Roe MT, et al. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With the Guidelines). Circ Cardiovasc Qual Outcomes. 2017;10(12):e003443. doi:10.1161/CIRCOUTCOMES.116.003443
- Gerbaud E, Arabucki F, Nivet H, et al. OCT and CMR for the Diagnosis of Patients Presenting With MINOCA and Suspected Epicardial Causes. JACC Cardiovasc Imaging. 2020;13(12):2619-2631. doi:10.1016/j.jcmg.2020.05.045
- Hayes SN, Kim ESH, Saw J, et al. Spontaneous Coronary Artery Dissection: Current State of the Science: A Scientific Statement From the American Heart Association. Circulation. 2018;137(19):e523-e557. doi:10.1161/CIR.0000000000000564
- Buda KG, Mallick S, Kohl LP. Myocardial infarction with nonobstructive coronary arteries: Current management strategies. Cleve Clin J Med. 2024;91(12):743-753. Published 2024 Dec 2. doi:10.3949/ccjm.91a.19127
- Lindahl B, Baron T, Erlinge D, et al. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation. 2017;135(16):1481-1489. doi:10.1161/CIRCULATIONAHA.116.026336
- Smilowitz NR, Dubner R, Hellkamp AS, Widmer RJ, Reynolds HR. Variability of discharge medical therapy for secondary prevention among patients with myocardial infarction with non-obstructive coronary arteries (MINOCA) in the United States. PLoS One. 2021;16(8):e0255462. Published 2021 Aug 2. doi:10.1371/journal.pone.0255462