
Have you ever stood in the grocery store aisle, looking at all the different bottles of oil, and felt totally lost? One day, you hear that butter is back and healthy. The next day, a video on the internet says seed oils are “toxic” and will make you sick. Then, someone else says extra virgin olive oil is the only “superfood” you should ever eat.
It feels like the rules for health change every single week. It is like trying to play a game where the referee keeps changing the score while the clock is running! This confusion is enough to make anyone want to give up and just pick whichever bottle has the prettiest label.
This confusion stops today. We are going to look at the facts from a major 2026 scientific review called The Lipid Debate. This report looked at all the best studies to find the truth about seed oils, olive oil, and your heart. We are going to clear up the “Seed Oil vs. Olive Oil” fight once and for all using real science. By the time you finish reading, you will know exactly what to put in your frying pan and why.
1. Seed Oils Aren’t the “Villains” They’re Made Out to Be
You might have heard people call oils like soybean, corn, or canola “toxic.” They often use the name “industrial seed oils” to make them sound like something that belongs in a car engine, not a kitchen. But when scientists look at these oils on their own, they do not find anything “poisonous” about them.
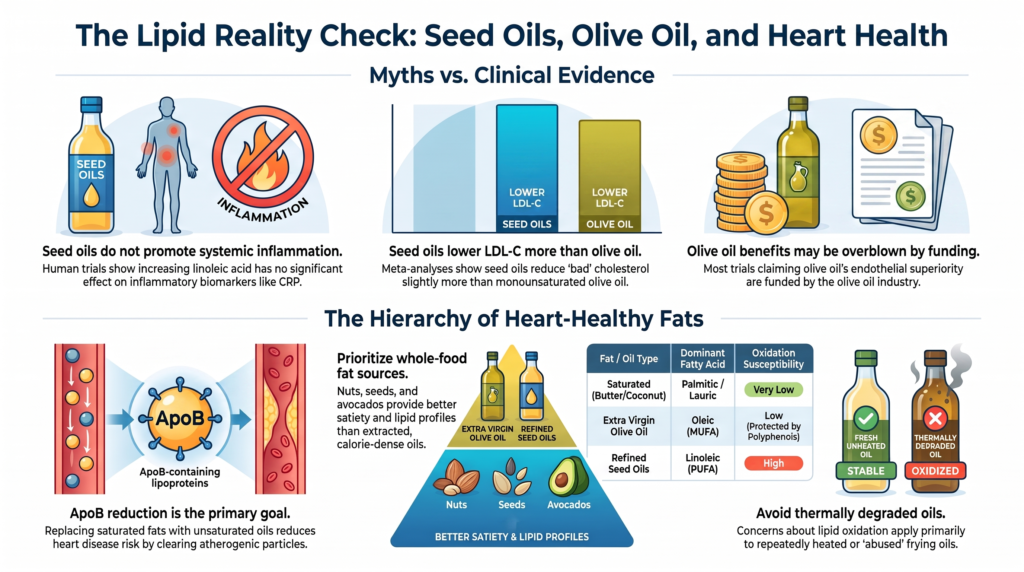
In fact, when these oils are fresh and used to replace animal fats like butter, they do something very good for your heart. They help lower the “bad” stuff in your blood called LDL-C and ApoB.
To understand why this matters, think of your liver like a big cleaning center and your blood like a highway. Your blood has “delivery trucks” (called ApoB particles) that carry fat around. If you have too many of these trucks on the road, they can crash into your blood pipe walls (your arteries) and cause a “traffic jam.” Over many years, these traffic jams lead to heart attacks.
When you eat seed oils instead of butter or coconut oil, it is like giving your liver a better set of instructions. These oils help the liver “open its doors” wider. Scientists call these doors “LDL receptors.” By opening these doors, the liver can pull the delivery trucks out of the blood and clear the highway.
The 2026 science review is very clear about this:
“Compared with butter and coconut oil, seed oils consistently lower low-density lipoprotein cholesterol (LDL-C) and ApoB.”
This is surprising to many people because we are taught that “processed” always means “bad.” While these oils are often found in junk food, the oils themselves are actually heart-friendly. When they replace saturated fats, they keep your “trash particles” (ApoB) low. Since ApoB is the main thing that starts heart disease, lowering it is the most important job your food can do.
2. The Omega-6 “Inflammation” Theory Doesn’t Hold Water
The biggest fear about seed oils is a specific fat they contain called “Omega-6” (or Linoleic Acid). Many people worry that if you eat it, it turns into “fire” inside your body. This “fire” is called inflammation. People claim this fire spreads through your body and makes you sick.
However, the science shows that our bodies are much smarter than a simple fireplace. Just because you eat Omega-6 does not mean your body turns it all into “fire.” In adults, only a tiny amount—about 0.3% to 0.6%—of this fat actually changes into the chemicals that could cause inflammation.
Think of it like this: if a delivery truck drops off a huge pile of wood in your driveway, it does not mean your whole house is going to catch on fire. You need a match and a reason to start that fire. Your body keeps a very tight balance. It uses most of that fat for energy or stores it safely. It does not just turn it all into inflammation automatically.
Scientists have done many tests on real people to see if eating more Omega-6 raises “inflammatory markers” like something called CRP. The result? It did not. Even when people ate much more Omega-6, their bodies stayed calm. The “fire” never happened. The body actually uses some of these fats to stop inflammation and heal itself. The idea that seed oils cause a “fire” in your body is a myth that does not match what happens in real human trials.
3. The Olive Oil “Halo” Might Be Partially Built on Marketing
Extra virgin olive oil (EVOO) has a “halo.” Most people think it is a perfect food that can do no wrong. But science shows it might not be as magical as the commercials say.
Scientists use a “flexibility test” for your blood pipes called FMD. When your blood pipes are flexible, they can open wide to let blood flow easily. One famous study found that after people ate a meal with olive oil, their blood pipes became 31% less flexible for a few hours. This is the same thing that happens with other oils. The fat in olive oil did not protect the blood pipes from getting a bit stiff after the meal.
It is important to know that this stiffness is a “surrogate marker.” That means it is a sign of how the body reacts right now, but it isn’t a heart attack. The stiffness usually lasts for 2 to 4 hours and then goes away. The long-term score—your ApoB levels—matters much more for your life.
So, why do we think olive oil is so much better? A lot of it comes down to who pays for the studies.
| Oil Type | Main Fat Source | Industry Funding | Effect on LDL-C (Bad Stuff) |
| Extra Virgin Olive Oil | Monounsaturated | Very High (Paid for by olive oil trade groups) | Lowers LDL-C, but less than seed oils |
| Refined Seed Oils | Polyunsaturated | Moderate (Paid for by soybean/corn groups) | Best at lowering LDL-C (4.2 mg/dL better than olive oil) |
| Butter / Coconut Oil | Saturated | Generally Independent | Raises LDL-C and ApoB |
When we look at the science, we have to be fair. Both sides have “skin in the game.” Seed oil research is often paid for by soybean and corn groups. Olive oil research is paid for by olive oil trade groups. This “symmetry” means we should look at both with a careful eye.
Also, olive oil seems to work best when it is eaten with vegetables. This is because the antioxidants in the veggies help stop the “stiffness” from happening. This explains why the Mediterranean Diet is so healthy: it isn’t just the oil, it is the “whole package” of healthy food.
4. All Liquid Oils are Like “Fast Food” for Your Arteries
This might be the most important takeaway: the biggest problem isn’t the name on the bottle, but the fact that it is a bottled oil at all.
Think about the difference between a whole orange and a glass of orange juice. When you eat the orange, your body has to work to break it down. The sugar enters your blood slowly because of the fiber. But when you drink the juice, the sugar hits you like a tidal wave.
Oil is just like “fat juice.” When companies make oil, they strip away the “walls” of the food. They take away the fiber and the cell membranes that hold the fat in place. Because these oils are liquids, they are absorbed by your gut very fast.
When you eat any extracted oil—even the expensive ones—the fat hits your blood like a “tidal wave” rather than a “slow trickle.” This “surge” of fat causes temporary stress to your blood pipes. It doesn’t matter if the oil came from an olive or a sunflower. Because it is a liquid that is missing its “whole food” package, it causes a few hours of stress every time you eat it.
We also have to remember how “heavy” oil is. A single tablespoon of any oil has 120 calories. That is a lot of energy in a tiny package! Because oil does not have fiber to fill you up, it is very easy to eat way too much of it without feeling full.
5. Your Heart Prefers the “Whole Package”
If you want to give your heart the very best, you should look for “Whole-Food Fat Sources.” This means eating things like:
- Walnuts, almonds, and pecans
- Sunflower seeds, chia seeds, and flax seeds
- Fresh avocados
- Whole olives
When fat is still inside its “whole food package,” it has a built-in “wall.” This wall is made of fiber and cell membranes. It acts as a physical fence. Your body has to work hard to get past that fence to grab the fat. This means the fat enters your blood as a “slow trickle” over many hours.
Science shows this makes a massive difference. One major review looked at 61 different studies with 2,582 people. It found that eating about 60 grams (two small handfuls) of whole tree nuts a day was amazing for the heart. These whole nuts lowered “trash particles” (ApoB) even better than just using isolated oils.
In one study, people who ate whole walnuts had much better blood pipe flexibility than people who just used olive oil. The whole walnut has fiber, protein, and special nutrients that the oil leaves behind. While using oil for cooking is “fine,” the whole food version is the gold standard for your health.
Conclusion: The Big Picture for Your Plate
So, what should you do when you are standing in that oil aisle? Here is the simple summary of what the 2026 review actually says:
- Lower your ApoB: Replacing animal fats like butter with plant oils (like olive or seed oils) is a win for your heart. It clears the “delivery trucks” out of your blood.
- Don’t fear the “fire”: You don’t need to worry about Omega-6 causing inflammation. That fear is not supported by human trials.
- Check the LDL-C: Remember that seed oils actually lower bad cholesterol about 4.2 mg/dL more than olive oil does. Both are better than butter!
- Go “Whole” first: Try to get most of your fats from nuts, seeds, and avocados. They have the “walls” that keep the fat from hitting your blood too fast.
- Avoid “abused” oil: The only time seed oils are truly a problem is when they are “broken.” This happens when they are reheated over and over again in deep fryers. This heat creates “broken oil pieces” called aldehydes that can hurt your body. Fresh oil is fine; old, “abused” restaurant oil is not.
Now that you know the “inflammation” fear was a myth and the “halo” on olive oil is partly marketing, will you focus more on the source of your fats (whole vs. bottled) rather than just the name on the label? Your heart—and your blood pipes—will thank you for choosing the “slow trickle” of whole foods!
DEEP DIVE
Seed Oils, Added Oils, and Cardiovascular Health
A Critical Scientific Review of Seed Oils Versus Olive Oil, Saturated Fat, and Whole-Food Fat Sources
Abstract
The dietary fat debate has evolved from a low-fat paradigm to a lipid-specific one. Historically, guidelines advised replacing saturated fatty acids with polyunsaturated fatty acids to lower serum cholesterol and prevent coronary heart disease. Over the past decade this guidance has been challenged by the hypothesis that industrial seed oils rich in omega-6 linoleic acid promote systemic inflammation and lipid peroxidation, alongside growing interest in the cardiovascular benefits of extra virgin olive oil and whole-food fat matrices. This review evaluates the physiological, mechanistic, and clinical trial evidence, treating apolipoprotein B (ApoB)-containing lipoproteins as the causal driver of atherosclerosis. Throughout, a deliberate distinction is drawn between mechanistic and surrogate markers, such as flow-mediated dilation and inflammatory biomarkers, and hard clinical endpoints such as myocardial infarction, stroke, and cardiovascular death. Every quantitative claim herein is drawn from primary peer-reviewed literature; claims that could not be verified against a primary source have been removed.
1. Introduction
The nutritional debate surrounding dietary fat has shifted from a simple low-fat model toward a complex, lipid-specific analysis. Public health guidelines historically recommended substituting saturated fatty acids (SFAs) with polyunsaturated fatty acids (PUFAs) to reduce serum total cholesterol (TC) and prevent coronary heart disease (CHD). Over the past decade this guidance has been challenged by the hypothesis that industrial seed oils rich in omega-6 linoleic acid (LA, 18:2n-6) promote chronic systemic inflammation and lipid peroxidation. Concurrently, evidence has accumulated for the cardiovascular benefits of extra virgin olive oil (EVOO) and lipid matrices derived from whole foods. [1]
This review provides a balanced evaluation of unrefined and refined seed oils and contrasts them with EVOO, refined olive oil, SFAs, and whole-food fat sources. Central to the analysis is the role of ApoB-containing lipoproteins as the causal drivers of atherosclerosis, while examining whether the postprandial and vascular effects of extracted fats contribute to risk independently of their effects on circulating lipids. [2], [3]
2. Are Seed Oils Uniquely Harmful?
The hypothesis that seed oils rich in linoleic acid (soybean, corn, sunflower, safflower, canola, cottonseed, grapeseed, and rice bran oils) possess unique adverse effects beyond those of other refined lipids remains under active study. The concern is rooted in chemical structure: PUFAs contain multiple double bonds separated by bis-allylic methylene groups, making them susceptible to hydrogen abstraction and lipid peroxidation. [6]
In modern diets these oils are consumed largely as ingredients in processed and ultra-processed food matrices, which confounds observational studies because the effects of refined seed oils are difficult to isolate from those of refined carbohydrate, high sodium, and low fiber.
When evaluated as isolated dietary components in controlled trials, seed oils do not exhibit unique toxicities. Instead they show predictable lipid-modulating effects based on their fatty acid profiles. Compared with butter and coconut oil, seed oils consistently lower low-density lipoprotein cholesterol (LDL-C) and ApoB. [4], [5]
2.1 Fatty Acid Profiles and Oxidative Stability
The fatty acid profiles and relative oxidative stabilities of the major added fats are summarized in Table 1. Susceptibility to autoxidation rises with the number of double bonds, so saturated and monounsaturated fats are far more oxidatively stable than polyunsaturated seed oils. Conventional high-linoleic seed oils and their high-oleic cultivars are chemically distinct: high-oleic sunflower, safflower, and soybean oils are dominated by monounsaturated oleic acid and are correspondingly more stable than their conventional high-linoleic counterparts. [6]
| Fat / Oil | Primary Class | Dominant Fatty Acid(s) | Double Bonds | Oxidation Susceptibility |
| Coconut oil | Saturated | Lauric (12:0), myristic (14:0) | 0 | Very low |
| Butter | Saturated | Palmitic (16:0), stearic (18:0) | 0 | Very low |
| Extra virgin olive oil | Monounsaturated | Oleic (18:1n-9) | 1 | Low (protected by polyphenols) |
| Canola oil | MUFA / PUFA | Oleic (18:1n-9), linoleic (18:2n-6), alpha-linolenic (18:3n-3) | 1 to 3 | Moderate |
| Soybean oil | Polyunsaturated | Linoleic (18:2n-6) | 2 | High |
| Corn oil | Polyunsaturated | Linoleic (18:2n-6) | 2 | High |
| Safflower (high-linoleic) | Polyunsaturated | Linoleic (18:2n-6) | 2 | Very high |
| Safflower (high-oleic) | Monounsaturated | Oleic (18:1n-9) | 1 | Low |
Table 1. Fatty acid composition and relative oxidative stability of major added fats. Compositional data reflect standard lipid chemistry references.
2.2 Industry Funding and Interpretation
Evaluation of the dietary fat literature is complicated by the prevalence of industry-funded nutrition research. A methodological analysis of beverage studies found that industry sponsorship was strongly associated with conclusions favorable to the sponsor; among interventional studies, the odds ratio for a favorable versus unfavorable conclusion comparing all-industry to no-industry funding was 7.61 (95% CI 1.27 to 45.73), and none of the sixteen all-industry interventional studies reported an unfavorable conclusion. [7]
That analysis concerned beverages rather than dietary fats, and no fat-specific odds ratio can be derived from it. It is cited here only to illustrate the general direction of funding bias. Consistency requires acknowledging that this scrutiny applies symmetrically across the fat debate: seed oil research has been supported by soybean, canola, and corn commodity interests, and olive oil research has been supported by olive oil trade organizations and producers, an industry of comparable commercial scale. Commercial sponsorship does not by itself invalidate a study, but it underscores the value of replication by independent, non-commercially funded research on all sides of the debate. [7]
3. Is the Principal Issue Added Oils Rather than Seed Oils?
An alternative hypothesis holds that the primary determinant of postprandial vascular dysfunction is the consumption of extracted, purified oils of any type, including olive oil, rather than the specific fatty acid profile of seed oils. Under this model, mechanical or chemical extraction strips lipids of their protective cellular structures, fibers, and micronutrient matrices, converting them into highly bioavailable, calorie-dense liquids. [3]
Extracted oils are more rapidly absorbed than intact food matrices in the upper gastrointestinal tract, producing a swift postprandial rise in circulating chylomicrons and triglyceride-rich lipoproteins. This can trigger transient oxidative stress and endothelial dysfunction. Consuming fats within whole-food matrices such as whole olives, soybeans, avocados, nuts, or seeds yields a slower, more controlled absorption profile, because dietary fiber, phytosterols, and intact cell membranes act as a physical barrier that slows lipase access. [3], [8]
3.1 Mechanistic Impact of Added Lipids on Vascular Physiology
Several interrelated pathways have been proposed by which extracted oils may affect vascular health. These are mechanistic proposals supported by postprandial physiology rather than by hard-outcome trials, and are presented as such. [3]
- Nitric oxide and endothelial function: Large postprandial lipid surges are proposed to increase superoxide production and reduce nitric oxide bioavailability, causing transient vasoconstrictive impairment. In one controlled human study, antioxidant vitamins C and E attenuated the postprandial impairment by 71%, implicating oxidative stress in the response. [8]
- Lipoprotein entry and retention: Postprandial changes may increase endothelial permeability and facilitate entry of ApoB-containing lipoproteins into the subendothelial matrix, the initiating step in atherogenesis. [2], [3]
- Arterial stiffness: Long-term markers of arterial stiffness appear to change minimally after short-term plant oil interventions, suggesting structural vascular change requires prolonged exposure. This remains a proposed mechanism pending dedicated primary confirmation.
The available mechanistic evidence raises the possibility that extracted oils, irrespective of fatty acid composition, may contribute to transient postprandial endothelial dysfunction. Repeated postprandial endothelial dysfunction represents a biologically plausible mechanism deserving further investigation. Although biologically plausible, no human trial has demonstrated that repeated transient FMD impairment independently accelerates plaque progression after adjustment for ApoB exposure, and no trial has directly shown this pathway progressing to plaque in humans. [3]
4. Flow-Mediated Dilation and Endothelial Function
Flow-mediated dilation (FMD) of the brachial artery is a validated surrogate of nitric oxide-dependent endothelial function, and impaired FMD is associated with future cardiovascular events. It is important to state plainly that FMD is a surrogate endpoint, not a clinical endpoint: it measures a physiological property of the vasculature, and a change in FMD does not by itself constitute a heart attack, stroke, or death prevented. Its value lies in mechanistic insight, not in quantifying clinical benefit. [8]
4.1 Postprandial Endothelial Responses to Lipids
A systematic review and meta-analysis of the acute effects of a single high-fat meal on endothelial function (131 studies, 90 in the quantitative synthesis) found statistically significant postprandial reductions in brachial artery FMD. [3]
- At 2 hours: FMD decreased by 1.02 percentage points (95% CI -1.34 to -0.70; P < 0.01). [3]
- At 3 hours: FMD decreased by 1.04 percentage points (95% CI -1.48 to -0.59; P < 0.001). [3]
- At 4 hours: FMD decreased by 1.19 percentage points (95% CI -1.53 to -0.84; P < 0.01). [3]
The percentage of energy from fat was inversely associated with the change in FMD at 3 hours (P < 0.01), consistent with a triglyceride-linked, transient oxidative mechanism. [3]
4.2 The Olive Oil FMD Paradox
A key observation in vascular biology is the olive oil FMD paradox described by Vogel and colleagues. Ten healthy, normolipidemic subjects consumed meals of 900 kcal containing 50 g of fat from different sources. [8]
The olive oil meal reduced postprandial FMD by 31%, from 14.3% to 9.9% (P = 0.008), whereas canola oil and salmon meals produced no significant decline. An inverse correlation was observed between the postprandial change in serum triglycerides and the change in FMD (r = -0.47; P < 0.05). When the olive oil meal was accompanied by antioxidant-rich foods or by vitamins C and E, the reduction was substantially prevented (by 65% and 71%, respectively). This indicates that the monounsaturated oleic acid backbone alone does not protect the endothelium from postprandial lipid-induced oxidative stress. Although informative mechanistically, the experimental meal contained approximately 50 g of fat, considerably greater than a typical single-meal fat intake for many individuals, so the magnitude of the response should not be extrapolated directly to habitual consumption. [8]
The preservation of endothelial function by extra virgin olive oil is often attributed to its hydrophilic secoiridoid phenolics, including hydroxytyrosol, oleuropein, oleocanthal, and oleacein, which act in vitro as free radical scavengers. This attribution should be treated with strong caution, and this review does not present it as reliable. The randomized trials reporting that high-polyphenol EVOO improves postprandial flow-mediated dilation are almost uniformly funded or materially supported by the olive oil industry. The most cited positive postprandial trial was funded by an extra virgin olive oil producer that supplied the study oil; the widely cited EUROLIVE program and several confirmatory phenolic trials are likewise olive-oil-industry-linked. By contrast, the cleanest relatively independent test of a phenol-specific effect on LDL oxidizability found no benefit beyond a polyphenol-free control oil. The positive FMD literature is therefore small, heterogeneous, and dominated by sponsor-conflicted studies, while the more independent evidence is null or mixed. On this basis the claim that olive oil polyphenols independently improve human endothelial function cannot presently be relied upon, and it should not be used to assert a cardioprotective advantage for olive oil. [17]
| Fat / Oil | Fatty Acid Backbone | Secondary Components | Postprandial FMD Effect |
| Butter | SFA (16:0, 18:0) | Cholesterol | Reduction |
| Refined seed oils | PUFA (18:2n-6) | Tocopherols (variable) | Transient reduction |
| Refined olive oil | MUFA (18:1n-9) | Very low polyphenols | Transient reduction |
| Extra virgin olive oil | MUFA (18:1n-9) | Secoiridoid polyphenols | Reported benefit vs refined oil, but positive trials are industry-funded and unreliable |
| Canola oil | MUFA (18:1n-9) | Phytosterols, ALA (18:3n-3) | No significant reduction |
Table 2. Reported postprandial flow-mediated dilation effects of major fat sources. Directional effects reflect the cited controlled studies; magnitudes vary by meal composition. FMD is a surrogate marker.
5. Omega-6 Fatty Acid Biology and Metabolism
To evaluate the hypothesis that seed oils promote systemic inflammation, the metabolic fate of linoleic acid (18:2n-6) must be examined. LA undergoes enzymatic conversion via a shared cascade of desaturation and elongation enzymes, ultimately yielding arachidonic acid (AA, 20:4n-6), the substrate for eicosanoid synthesis through the cyclooxygenase, lipoxygenase, and cytochrome P450 pathways. [9]
The omega-6 hypothesis proposes that high dietary LA enriches membranes with AA, overproducing pro-inflammatory mediators. Human stable-isotope tracer studies show this model is largely inaccurate in adults. The fractional conversion of dietary LA to AA is estimated at only 0.3% to 0.6%, reflecting low activity of the rate-limiting delta-6-desaturase in adult human tissue. [9], [10]
A systematic review of human interventions found that decreasing dietary LA by up to 90% was not significantly correlated with the AA content of plasma or serum phospholipids (P = 0.39), and increasing dietary LA severalfold was likewise uncorrelated with AA (P = 0.72). Excess dietary LA is primarily beta-oxidized for energy or stored in adipose tissue rather than converted to AA. [9]
Arachidonic acid metabolism is also intrinsically balanced. Established eicosanoid biochemistry shows that AA is the precursor not only to pro-inflammatory mediators but also to prostacyclin, a vasodilator and inhibitor of platelet activation, and to lipoxins, which are specialized pro-resolving mediators that actively down-regulate inflammation. A simple model in which more dietary LA yields uniformly more inflammation is therefore inconsistent with the underlying biochemistry.
6. Does Omega-6 Increase Chronic Inflammation?
A systematic review of randomized controlled trials examining dietary LA and chronic inflammation in healthy, non-infant populations found no evidence of harm. Across trials, increasing dietary LA had no significant effect on circulating C-reactive protein (CRP), fibrinogen, plasminogen activator inhibitor-1, interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-alpha), or soluble adhesion molecules. [11]
The clinical evidence therefore does not support the hypothesis that high dietary omega-6 intake promotes systemic inflammation in humans. This conclusion rests on controlled human trials with objective biomarker endpoints rather than on mechanistic extrapolation from eicosanoid pathways. [11]
For transparency, and consistent with the funding considerations in Section 2, the linoleic acid inflammation review was supported by an unrestricted grant from an industry technical committee, and the high-oleic oil review discussed below was funded by a commodity board. Their conclusions nonetheless align with the independent Cochrane and network meta-analytic evidence presented in Sections 7 and 8. [11]
7. Seed Oils Versus Saturated Fat
7.1 Metabolic and Lipid Effects
Replacing saturated fats with polyunsaturated seed oils substantially lowers atherogenic lipids. A network meta-analysis of 54 randomized trials ranked oils and solid fats by their effects on blood lipids. Safflower oil had the highest probability of reducing LDL-C (SUCRA 82%) and total cholesterol (SUCRA 90%), followed by rapeseed (canola) oil (SUCRA 76% for LDL-C, 85% for total cholesterol). Unsaturated oils reduced LDL-C by roughly 0.23 to 0.42 mmol/L relative to butter. This effect is driven primarily by up-regulation of hepatic LDL receptors, which increases clearance of circulating ApoB-containing particles. [4]
A systematic review of high-oleic vegetable oil substitutions quantified the ApoB effect directly: replacing saturated fats with high-oleic oils reduced total cholesterol by 8.0%, LDL-C by 10.9%, and ApoB by 7.9% (all P < 0.05). The relevant intervention is replacement rather than unrestricted addition: the evidence supports substituting unsaturated fat for saturated fat within the range of roughly 5 to 10 percent of total energy intake, not the unlimited addition of oils on top of an existing diet. [5]
7.2 Clinical Cardiovascular Outcomes
An updated Cochrane systematic review of reducing saturated fat intake pooled 15 randomized controlled trials comprising 56,675 participants who reduced saturated fat for at least two years. Reducing saturated fat produced a statistically significant 17% reduction in combined cardiovascular events (risk ratio 0.83; 95% CI 0.70 to 0.98; I-squared 67%). [18]
Subgroup analysis and meta-regression indicated the benefit was driven by replacing saturated fat with polyunsaturated fat or high-quality carbohydrate, with greater cholesterol reductions predicting greater protection. The number needed to treat was 56 in primary prevention and 53 in secondary prevention. [18]
Despite the reduction in combined events, reducing saturated fat had little or no effect on all-cause mortality (55,858 participants, 11 trials) or cardiovascular mortality (53,421 participants, 10 trials), both with moderate-quality evidence. This dissociation between event reduction and mortality is itself important and is discussed further in Section 12. [18]
7.3 Critical Re-Evaluation of Historical Controversies
Critics of the diet-heart hypothesis frequently cite recovered data from two historical trials re-analyzed by Ramsden and colleagues.
- Minnesota Coronary Experiment: A double-blind randomized trial of 9,423 institutionalized participants comparing a diet in which saturated fat was replaced with corn oil against a saturated-fat control. The corn oil intervention lowered serum cholesterol by 13.8% versus 1.0% in controls (P < 0.001), yet produced no survival benefit. In covariate-adjusted models, a 30 mg/dL reduction in serum cholesterol was associated with a 22% higher risk of death (hazard ratio 1.22; 95% CI 1.14 to 1.32; P < 0.001). [13]
- Sydney Diet Heart Study: A randomized trial in 458 men with a recent coronary event found that replacing saturated fat with safflower oil increased all-cause mortality (17.6% versus 11.8%; hazard ratio 1.62; 95% CI 1.00 to 2.64), cardiovascular mortality (hazard ratio 1.70; 95% CI 1.03 to 2.80), and coronary mortality (hazard ratio 1.74; 95% CI 1.04 to 2.92). [14]
Both trials have important limitations that constrain their relevance to modern recommendations. To reach very high linoleic acid intakes, investigators used synthetic foods that removed marine and plant omega-3 fats, producing diets deficient in essential omega-3 PUFAs. The margarines used contained industrial trans-fatty acids now known to be atherogenic. Both studies also suffered severe attrition and short participant retention. [13], [14]
8. Seed Oils Versus Olive Oil
8.1 Direct Lipid-Modulating Effects
Because of their higher polyunsaturated content, linoleic-acid-rich seed oils lower total cholesterol and LDL-C somewhat more than monounsaturated-rich olive oil. A meta-analysis of 27 randomized placebo-controlled trials (1,089 participants) found that olive oil reduced LDL-C less than other plant oils by a weighted mean difference of 4.2 mg/dL (95% CI 1.4 to 7.01; P = 0.003) and reduced total cholesterol less by 6.27 mg/dL (95% CI 2.8 to 10.6). Although statistically significant, the magnitude of this LDL-C difference relative to olive oil is modest, and readers should not interpret it as a large clinical separation between the two. [15]
Conversely, olive oil raised high-density lipoprotein cholesterol (HDL-C) more than other plant oils, an effect that was significant in trials longer than 30 days (weighted mean difference 1.77 mg/dL; 95% CI 0.28 to 3.27; P = 0.02). [15]
8.2 Olive Oil Grades
The term olive oil encompasses several distinct products that readers frequently conflate. Virgin olive oils are produced by mechanical means without chemical treatment; extra virgin olive oil is the highest grade, meeting stricter sensory and free-acidity criteria and retaining the full complement of native polyphenols. Refined olive oil is virgin oil that has been chemically or physically refined to remove defects, a process that strips the great majority of its polyphenols while leaving the oleic acid backbone intact. Olive pomace oil is extracted from the residual paste using solvents and then refined. Because the vascular and antioxidant advantages of olive oil track its polyphenol content rather than its oleic acid content, these grades are not interchangeable, and evidence generated with high-polyphenol extra virgin oil should not be assumed to apply to refined or pomace grades. [17]
8.3 Vascular, Endothelial, and Inflammatory Profiles
Olive oil is sometimes said to outperform refined seed oils on vascular inflammation and endothelial function, but that claim rests on a compromised evidence base and is not relied upon here. A meta-analysis of 30 randomized controlled trials in 3,106 participants reported that olive oil consumption was associated with lower IL-6 (mean difference -0.29 pg/mL; 95% CI -0.7 to -0.02), lower soluble E-selectin (mean difference -3.16; 95% CI -4.07 to -2.25), and higher FMD (mean difference 0.76%; 95% CI 0.27 to 1.24). These are surrogate markers, not clinical events, and the underlying trials are disproportionately olive-oil-industry-funded, including the leading positive postprandial FMD trial, which was financed by an olive oil producer. Because the positive endothelial findings cluster in sponsor-conflicted studies while more independent tests are null or mixed, no reliable conclusion of endothelial superiority for olive oil can be drawn, and the surrogate improvements should not be extrapolated to event reduction. [16]
8.4 Isolating the Contribution of Polyphenols
To determine whether the benefits of EVOO derive from its oleic acid backbone or its minor bioactive compounds, the EUROLIVE study fed 200 healthy men 25 mL/day of olive oils with low (2.7 mg/kg), medium (164 mg/kg), or high (366 mg/kg) polyphenol content in a randomized crossover design. HDL-C rose linearly with polyphenol content (change of +0.045 mmol/L at the highest dose; 95% CI 0.02 to 0.06), and oxidized LDL fell linearly (change of -3.21 U/L at the highest dose; 95% CI -5.1 to -0.8), while the low-polyphenol oil increased oxidized LDL. [17]
These dose-dependent findings underpin the European Union authorized health claim for olive oil polyphenols, which requires a minimum of 5 mg of hydroxytyrosol and its derivatives per 20 g of oil. This regulatory claim should not be mistaken for reliable evidence of clinical cardioprotection. EUROLIVE and the great majority of confirmatory phenolic and endothelial trials carry olive-oil-industry funding, so they cannot be read as independent confirmation, and at least one clean controlled trial found that phenol-fortified oil did not increase LDL-oxidation resistance beyond a polyphenol-free control oil. Because the supportive evidence is dominated by sponsor-conflicted studies and the more independent evidence is null or mixed, the polyphenol mechanism cannot be relied upon as a basis for recommending olive oil over other unsaturated fats. [17]
| Marker | Extra Virgin Olive Oil | Refined Olive Oil | Refined Seed Oils |
| LDL-C lowering | Moderate | Moderate | High |
| HDL-C effect | Increase | Minimal | Neutral or decrease |
| Oxidized LDL | Decrease | No significant effect | Variable / not consistently improved |
| Systemic inflammation (IL-6) | Reduction | No significant reduction | Neutral to variable |
| Postprandial FMD | Preserved or improved | Context-dependent transient reduction | Context-dependent transient reduction |
| Oxidative stability | High | Moderate | Low |
Table 3. Comparative lipid, oxidative, and vascular profiles of extra virgin olive oil, refined olive oil, and refined seed oils, based on the cited trials.
9. Whole Foods Versus Extracted Oils
Comparing extracted oils with their whole-food counterparts reveals differences in bioavailability, postprandial kinetics, and satiety. Extraction removes cellular structure and dietary fiber; in whole nuts, seeds, olives, and avocados the lipid remains within cell walls, limiting bioaccessibility so that a portion of fat passes unabsorbed into the lower gastrointestinal tract. [8], [24]
The whole-food form also carries measurable lipid benefit. A systematic review, meta-analysis, and dose-response of 61 controlled trials (2,582 participants) found that tree nut consumption lowered total cholesterol and LDL-C in a nonlinear fashion, with stronger effects above roughly 60 g/day, and lowered ApoB and triglycerides in a linear dose-response. This is consistent with the ApoB-centered framework of this review, since whole nuts reduce the atherogenic particle burden directly. [24]
Extracted oils are among the most calorie-dense foods in the diet, providing approximately 9 kcal/g, or roughly 120 kcal per tablespoon, with negligible fiber or protein. This density and lack of structural volume may produce less satiety per calorie and promote positive energy balance, which matters because excess adiposity is itself a cardiovascular risk factor. Olive oil, seed oil, and butter are all energy-dense, so any of them, consumed in excess, can contribute to weight gain independent of fatty acid quality.
Controlled human data support a functional difference between whole foods and their oils: walnuts preserved postprandial endothelial function relative to olive oil in patients with hypercholesterolemia, an effect attributed to their combined fatty acid, antioxidant, and L-arginine content. [22]
Whole-food fat sources consistently improve intermediate metabolic markers compared with isolated oils, including satiety per calorie, postprandial metabolism, and circulating ApoB, and possibly endothelial function. Randomized trials have not established, however, that they produce superior cardiovascular event reduction compared with high-quality dietary patterns containing unsaturated oils, because few long-term trials directly compare oil-free whole-food diets with oil-containing diets. The case for whole foods therefore rests on convergent intermediate evidence and biological plausibility, not on proven event reduction, and this distinction should be kept in view when translating mechanism into recommendation. [8], [24]
10. Lipid Oxidation during Processing, Storage, and Cooking
The rate of lipid autoxidation is proportional to the number of double bonds in the fatty acid chain, so PUFAs are highly susceptible to free radical attack. When refined high-PUFA seed oils are heated for prolonged periods, especially under repeated commercial frying conditions, they undergo thermal oxidation, hydrolysis, and polymerization. Oxidation is also accelerated by repeated fryer reuse, air and light exposure, and prolonged storage, and is retarded by dark glass, cool storage, and inert-gas flushing. [6], [12]
This degradation generates primary lipid hydroperoxides that decompose into reactive secondary products, including aldehydes such as malondialdehyde and 4-hydroxynonenal, and oxidized linoleic acid metabolites such as 9-HODE and 13-HODE. In humans, lowering dietary linoleic acid measurably reduces circulating bioactive oxidized linoleic acid metabolites, confirming a diet-responsive pathway. An interpretive caution applies throughout this literature: circulating oxidized-LDL and oxidized-metabolite measurements correlate with, but do not directly demonstrate, oxidation occurring within the arterial plaque itself, and the two should not be equated. [6], [23]
By contrast, monounsaturated and saturated fats have far fewer double bonds and lack vulnerable bis-allylic carbons, making them more resistant to thermal breakdown. These oxidation-product mechanisms are biologically plausible contributors to endothelial and mitochondrial stress, but the magnitude of their clinical contribution relative to circulating ApoB remains a proposed rather than an established pathway. A crucial distinction, frequently conflated in popular discussion, is that these concerns apply to repeatedly heated and thermally degraded oils, not to fresh, unheated seed oils; the oxidation products of abused frying oil are not a property of the fresh oil itself. [6], [12]
11. Endothelial Injury, Atherosclerosis, and the Primacy of ApoB
The vascular failure hypothesis proposes that repeated postprandial endothelial stress from extracted oils contributes over decades to increased endothelial permeability, lipoprotein entry, and vascular inflammation. Repeated transient endothelial dysfunction represents a biologically plausible mechanism that could contribute to long-term vascular injury, although direct clinical evidence demonstrating this pathway in humans remains limited. It is best regarded as a contributory hypothesis, not an established initiating cause. [3]
Vascular biology establishes that endothelial dysfunction alone cannot initiate atherosclerosis in the absence of circulating ApoB-containing lipoproteins. The European Atherosclerosis Society consensus concludes that the retention and accumulation of cholesterol-rich ApoB-containing lipoproteins within the arterial intima is the initiating event of atherogenesis, with risk accruing in a dose-dependent manner. ApoB is generally a more direct measure of circulating atherogenic particle number than LDL cholesterol, because each atherogenic particle carries a single ApoB molecule. Any dietary change that lowers circulating ApoB reduces the particle burden available to penetrate and be retained in the arterial wall, which explains why the lipid-lowering effect of replacing saturated fat with unsaturated oils appears to override transient postprandial stress in long-term trials. Mendelian randomization studies reinforce this framework, showing that genetically lower LDL and ApoB reduce cardiovascular risk irrespective of the mechanism by which they are lowered. [2], [21]
12. Clinical Outcomes and Population Subgroups
Long-term trials and cohorts show that substituting saturated fat with polyunsaturated plant oils lowers the risk of combined cardiovascular events, an effect strongly correlated with the magnitude of cholesterol lowering, supporting reduction of circulating ApoB as the primary mechanism. The effect on stroke and on total mortality is less pronounced in pooled randomized data. [18], [21]
12.1 Olive Oil and the Mediterranean Pattern
For established coronary disease, the CORDIOPREV trial randomized 1,002 patients to a Mediterranean diet rich in EVOO or a low-fat diet over seven years. The primary composite endpoint occurred at 28.1 versus 37.7 events per 1,000 person-years, and multivariable-adjusted hazard ratios across models ranged from 0.719 (95% CI 0.541 to 0.957) to 0.753 (95% CI 0.568 to 0.998) in favor of the Mediterranean diet. Two interpretive caveats apply: the low-fat comparator reduced total fat only to roughly 32 percent of calories, short of a strict low-fat target, and the trial was funded by an olive-oil trade body, so the effect may partly reflect the comparator and should carry the same funding caution noted above. [20]
The landmark primary-prevention trial is PREDIMED, which randomized 7,447 high-risk participants to a Mediterranean diet supplemented with extra virgin olive oil, the same diet supplemented with nuts, or a reduced-fat control. In the republished intention-to-treat analysis, the adjusted hazard ratio for major cardiovascular events was 0.69 (95% CI 0.53 to 0.91) for the olive oil arm and 0.72 (95% CI 0.54 to 0.95) for the nut arm, roughly a 30% relative reduction. Three caveats are essential. First, the original 2013 report was retracted and republished in 2018 after a baseline-data audit found that randomization had been compromised for approximately 1,588 of the 7,447 participants (about 21 percent), including household members assigned en masse and a clinic randomized as a unit; the republished, clustering-adjusted analysis reached materially similar conclusions but is best regarded as quasi-randomized rather than strictly individually randomized. Second, the intervention was an entire Mediterranean dietary pattern, not olive oil in isolation, so the benefit cannot be attributed to olive oil alone. Third, the intervention oil was donated by the olive-oil trade, a funding entanglement that, consistent with the symmetry principle in Section 2.2, warrants the same caution applied to commodity-funded seed oil research. [19]
12.2 Absolute Risk Reduction and the Limits of Surrogate Markers
A recurring gap in discussions of dietary fat is the leap from surrogate markers to implied clinical benefit. Improvements in LDL-C, HDL-C, oxidized LDL, FMD, and IL-6 are meaningful mechanistically, but readers are ultimately concerned with heart attacks and deaths prevented, and the two do not always move in proportion. The clearest absolute figures come from the Cochrane saturated fat review, where the number needed to treat to prevent one cardiovascular event over the trial durations was 56 in primary prevention and 53 in secondary prevention, while all-cause and cardiovascular mortality were not significantly reduced. [18]
For olive oil specifically, no randomized trial has tested olive oil alone against a control for hard cardiovascular endpoints. The event-reduction evidence attributed to olive oil derives from whole-pattern Mediterranean diet trials such as PREDIMED and CORDIOPREV, in which olive oil was one component among many. Consequently, the precise absolute risk reduction attributable to olive oil as an isolated intervention is not known. Accordingly, estimates that olive oil alone reduces myocardial infarction by a specific percentage cannot presently be supported by randomized evidence. This is an honest limitation rather than a weakness of the underlying dietary advice. [19], [20]
12.3 Population Subgroups
For patients with familial hypercholesterolemia, who have genetically reduced LDL receptor function and high lifetime ApoB exposure, restricting saturated fat and substituting unsaturated plant oils maximizes LDL receptor activity and complements pharmacotherapy. In older adults, the relationship between serum cholesterol and survival is less linear, and aggressive dietary cholesterol lowering must be balanced against nutritional adequacy. Across subgroups, the unifying principle remains reduction of lifetime ApoB exposure. [2], [21]
13. Synthesis and Answers to Core Questions
- Are seed oils uniquely harmful compared with other added oils?
No. There is no high-quality evidence that unrefined or minimally processed seed oils possess unique harmful properties versus other refined extracted oils. When consumed as fresh, unheated lipids, they do not promote chronic inflammation or worsen metabolic health. The dominant confounder is their consumption within ultra-processed food matrices. [4], [11]
- Do omega-6 fatty acids increase chronic inflammation in humans?
No. Randomized controlled trials show that dietary linoleic acid does not increase circulating inflammatory biomarkers. Conversion of linoleic acid to arachidonic acid is only 0.3% to 0.6% and tightly regulated, and arachidonic acid gives rise to both pro-inflammatory and pro-resolving mediators. [9], [11]
- Do seed oils impair endothelial function differently from olive oil?
This cannot be reliably answered from the current evidence. Trials reporting that high-polyphenol EVOO preserves or improves postprandial FMD relative to refined oils are almost all funded or supplied by the olive oil industry, including the leading positive trial, whereas the cleanest more independent test showed no phenol-specific benefit. Refined seed oils and refined olive oil cause a transient FMD reduction linked to the acute triglyceride load, and the isolated oleic acid backbone is not protective. Given the industry-dominated and mixed evidence, no dependable difference in endothelial effect between olive oil and seed oils can be asserted, and FMD is in any case only a surrogate marker. [8], [17]
- Is the primary concern extracted oils regardless of fatty acid composition?
From a postprandial standpoint, extracted oils of all types are more rapidly absorbed than intact food matrices and can transiently impair endothelial function, and their high caloric density may produce less satiety per calorie. Whether this translates into long-term risk independent of ApoB lowering remains uncertain. High-polyphenol EVOO is sometimes proposed as a partial exception on the grounds that its antioxidant fraction counteracts lipid-induced endothelial stress, but that proposition rests largely on industry-funded trials and is not reliably established. [3], [8]
- Does replacing saturated fat with seed oils improve outcomes primarily through LDL-C and ApoB?
Yes. The benefit is driven by lowering atherogenic ApoB-containing lipoproteins. Saturated fats down-regulate hepatic LDL receptors, and replacing them with unsaturated oils up-regulates receptor activity and sustainably lowers circulating ApoB for as long as the dietary change is maintained. [5], [21]
- Do whole-food fat sources provide superior cardiovascular outcomes?
For intermediate metabolic markers, the evidence favors whole foods, and whole nuts lower ApoB directly. For hard clinical endpoints the evidence is limited, because few long-term randomized trials compare oil-free with oil-containing diets. [8], [24]
- What role does acute postprandial FMD impairment play in long-term atherosclerosis?
It is a reproducible marker of transient vascular stress but remains secondary to ApoB retention. Atherosclerosis cannot initiate without accumulation of ApoB-containing particles in the arterial wall, so the durable ApoB reduction from replacing saturated fat outweighs transient postprandial stress. [2], [21]
13.1 Evidence-Based Recommendations
The totality of primary evidence supports a dietary pattern that prioritizes replacing saturated fat with plant-derived unsaturated fats, particularly for those with elevated ApoB, familial hypercholesterolemia, or established coronary disease; treats olive oil and other unsaturated plant oils as reasonable substitutes for animal fat on the basis of their LDL and ApoB effects rather than any demonstrated endothelial or polyphenol advantage, since the evidence for the latter is dominated by industry funding and cannot be relied upon; favors whole-food fat sources such as nuts, seeds, avocados, olives, and fatty fish, which lower ApoB directly and improve satiety; and minimizes thermally degraded, repeatedly heated, or deep-fried oils. Where surrogate markers improve, the honest framing is that these are mechanistically favorable changes whose translation into event reduction is best evidenced for whole dietary patterns rather than for any single oil in isolation. [18], [24], [6]
References
- Sacks FM, Lichtenstein AH, Wu JHY, et al. Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation. 2017;136(3):e1-e23. doi:10.1161/CIR.0000000000000510
- Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459-2472. doi:10.1093/eurheartj/ehx144
- Fewkes JJ, Kellow NJ, Cowan SF, Williamson G, Dordevic AL. A single, high-fat meal adversely affects postprandial endothelial function: a systematic review and meta-analysis. Am J Clin Nutr. 2022;116(3):699-729. doi:10.1093/ajcn/nqac153
- Schwingshackl L, Bogensberger B, Benčič A, Knüppel S, Boeing H, Hoffmann G. Effects of oils and solid fats on blood lipids: a systematic review and network meta-analysis. J Lipid Res. 2018;59(9):1771-1782. doi:10.1194/jlr.P085522
- Huth PJ, Fulgoni VL 3rd, Larson BT. A systematic review of high-oleic vegetable oil substitutions for other fats and oils on cardiovascular disease risk factors: implications for novel high-oleic soybean oils. Adv Nutr. 2015;6(6):674-693. Published 2015 Nov 13. doi:10.3945/an.115.008979
- Grootveld M. Evidence-Based Challenges to the Continued Recommendation and Use of Peroxidatively-Susceptible Polyunsaturated Fatty Acid-Rich Culinary Oils for High-Temperature Frying Practises: Experimental Revelations Focused on Toxic Aldehydic Lipid Oxidation Products. Front Nutr. 2022;8:711640. Published 2022 Jan 5. doi:10.3389/fnut.2021.711640
- Lesser LI, Ebbeling CB, Goozner M, Wypij D, Ludwig DS. Relationship between funding source and conclusion among nutrition-related scientific articles. PLoS Med. 2007;4(1):e5. doi:10.1371/journal.pmed.0040005
- Vogel RA, Corretti MC, Plotnick GD. The postprandial effect of components of the Mediterranean diet on endothelial function. J Am Coll Cardiol. 2000;36(5):1455-1460. doi:10.1016/s0735-1097(00)00896-2
- Rett BS, Whelan J. Increasing dietary linoleic acid does not increase tissue arachidonic acid content in adults consuming Western-type diets: a systematic review. Nutr Metab (Lond). 2011;8:36. Published 2011 Jun 10. doi:10.1186/1743-7075-8-36
- Demmelmair H, Iser B, Rauh-Pfeiffer A, Koletzko B. Comparison of bolus versus fractionated oral applications of [13C]-linoleic acid in humans. Eur J Clin Invest. 1999;29(7):603-609. doi:10.1046/j.1365-2362.1999.00477.x
- Johnson GH, Fritsche K. Effect of dietary linoleic acid on markers of inflammation in healthy persons: a systematic review of randomized controlled trials. J Acad Nutr Diet. 2012;112(7):1029-1041.e10415. doi:10.1016/j.jand.2012.03.029
- Bazina N, Ahmed T, Almdaaf M, Abu Hallalah HMO, Jibia S. Chemical Changes in Deep-Fat Frying: Reaction Mechanisms, Oil Degradation, and Health Implications. Food Sci Nutr. 2025;13(10):e70969. Published 2025 Oct 13. doi:10.1002/fsn3.70969
- Ramsden CE, Zamora D, Majchrzak-Hong S, et al. Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73). BMJ. 2016;353:i1246. Published 2016 Apr 12. doi:10.1136/bmj.i1246
- Ramsden CE, Zamora D, Leelarthaepin B, et al. Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ. 2013;346:e8707. Published 2013 Feb 4. doi:10.1136/bmj.e8707
- Ghobadi S, Hassanzadeh-Rostami Z, Mohammadian F, et al. Comparison of blood lipid-lowering effects of olive oil and other plant oils: A systematic review and meta-analysis of 27 randomized placebo-controlled clinical trials. Crit Rev Food Sci Nutr. 2019;59(13):2110-2124. doi:10.1080/10408398.2018.1438349
- Schwingshackl L, Christoph M, Hoffmann G. Effects of Olive Oil on Markers of Inflammation and Endothelial Function-A Systematic Review and Meta-Analysis. Nutrients. 2015;7(9):7651-7675. Published 2015 Sep 11. doi:10.3390/nu7095356
- Covas MI, Nyyssönen K, Poulsen HE, et al. The effect of polyphenols in olive oil on heart disease risk factors: a randomized trial. Ann Intern Med. 2006;145(5):333-341. doi:10.7326/0003-4819-145-5-200609050-00006
- Hooper L, Martin N, Jimoh OF, Kirk C, Foster E, Abdelhamid AS. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev. 2020;8(8):CD011737. Published 2020 Aug 21. doi:10.1002/14651858.CD011737.pub3
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389
- Delgado-Lista J, Alcala-Diaz JF, Torres-Peña JD, et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. Lancet. 2022;399(10338):1876-1885. doi:10.1016/S0140-6736(22)00122-2
- Borén J, Chapman MJ, Krauss RM, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2020;41(24):2313-2330. doi:10.1093/eurheartj/ehz962
- Cortés B, Núñez I, Cofán M, et al. Acute effects of high-fat meals enriched with walnuts or olive oil on postprandial endothelial function. J Am Coll Cardiol. 2006;48(8):1666-1671. doi:10.1016/j.jacc.2006.06.057
- Ramsden CE, Ringel A, Feldstein AE, et al. Lowering dietary linoleic acid reduces bioactive oxidized linoleic acid metabolites in humans. Prostaglandins Leukot Essent Fatty Acids. 2012;87(4-5):135-141. doi:10.1016/j.plefa.2012.08.004
- Del Gobbo LC, Falk MC, Feldman R, Lewis K, Mozaffarian D. Effects of tree nuts on blood lipids, apolipoproteins, and blood pressure: systematic review, meta-analysis, and dose-response of 61 controlled intervention trials. Am J Clin Nutr. 2015;102(6):1347-1356. doi:10.3945/ajcn.115.110965