
1. Introduction: The “Magic Pill” That Changed the Rules
For many years, aspirin was seen as a “magic pill.” People thought of it almost like a daily vitamin for the heart. It was very common for adults to start taking a baby aspirin every day “just in case.” It seemed like a cheap and easy way to stop a heart attack or a stroke before it ever happened. Because aspirin is sold in every grocery store, it felt safe for everyone to use.
But the world of science never stays still. In the last few years, the rules for aspirin have changed a lot. New studies show that we need to be much more careful with this medicine. Aspirin is not just a supplement; it is a powerful drug that changes how your blood works.
Think of aspirin like a very sharp axe. If you are in the woods and need to chop down a tree to stay warm, that axe is a life-saver. It is exactly the right tool for a big job. But you would not walk around your living room carrying a sharp axe every day just to be safe. If you did, you might accidentally trip and cut yourself. You might even hurt someone else.
In the same way, aspirin is a great tool for some people, but it can be dangerous for others. New rules from heart experts tell us that for many healthy people, the risk of taking aspirin is now higher than the benefit. If you are taking it today, it is important to know which group you fall into.
2. The Big Switch: “Primary” vs. “Secondary” Prevention
The most important thing to learn is the difference between “Primary” and “Secondary” prevention. This is the single biggest rule in heart health today.
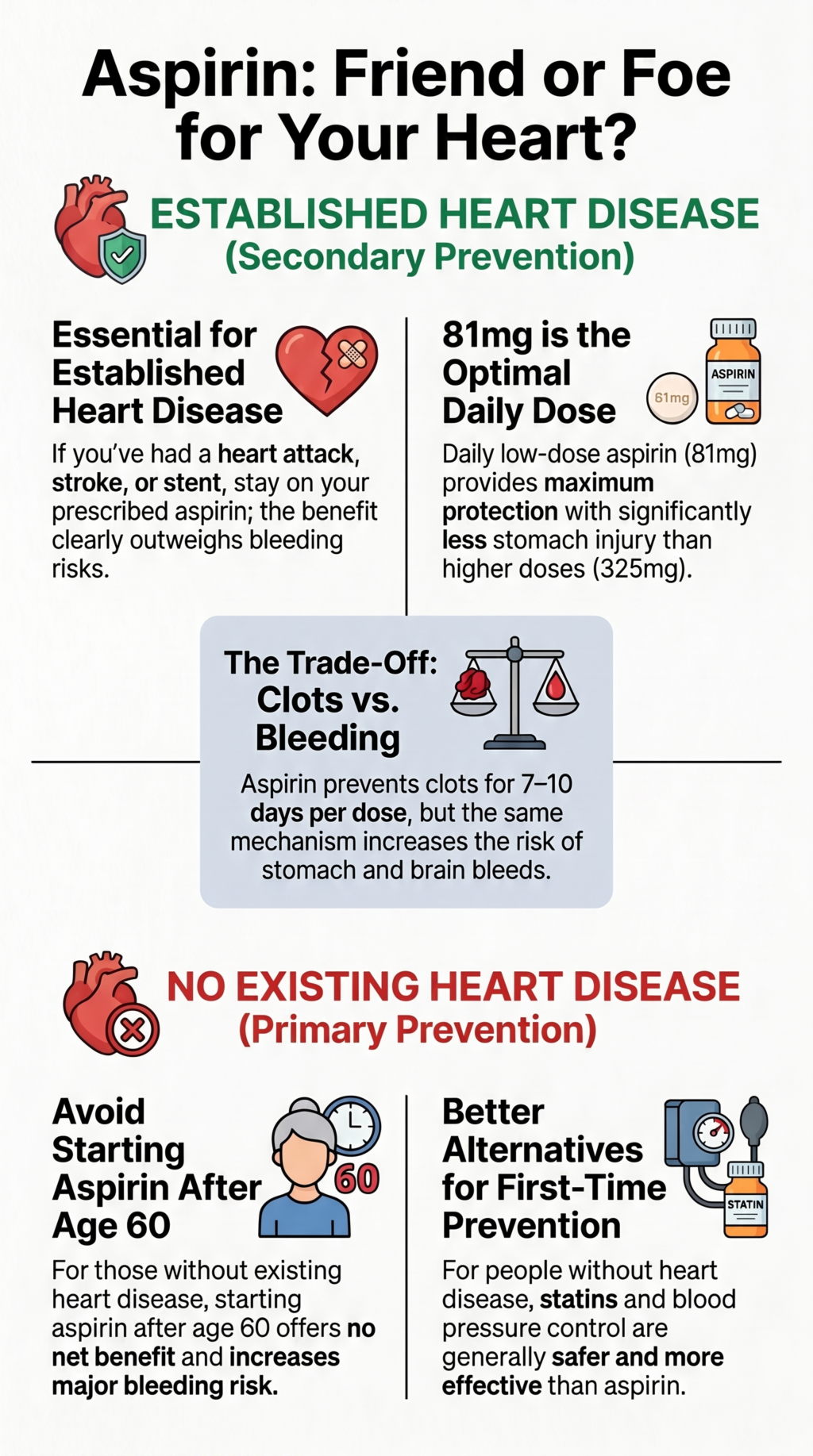
Secondary Prevention This group is for people who have already had heart trouble. If you have already had a heart attack or a stroke, you are in this group. This also includes people who have had a “mini-stroke” or surgery to fix their heart’s blood pipes, like a stent or a bypass. For these people, the pipes are already damaged. The risk of a second heart attack is very high. In this case, the benefit of aspirin is much bigger than the risk of bleeding.
Primary Prevention This group is for people who have never had a heart attack or a stroke. You might have high blood pressure or high cholesterol, but your heart pipes have not had a major “event” yet. You are taking aspirin to prevent your first heart attack. This is where the rules have changed the most.
For the Primary Prevention group, the “benefit-risk balance” is totally different. Because the chance of a heart attack is lower, the risk of dangerous bleeding becomes a much bigger deal.
Expert researchers have said:
“The benefit–risk balance of aspirin differs fundamentally between secondary prevention… and primary prevention. Conclusions in one setting do not transfer to the other.”
A Very Important Warning: If you are already taking aspirin because you have had a heart attack, stroke, or heart surgery, do not stop taking it. The new data about the risks of aspirin is mostly for people who have never had heart disease. If you are in the “Secondary” group, aspirin is still a lifesaver. Always talk to your doctor before you make any changes to your medicine.
3. Takeaway #1: The 60-Year-Old “Stop Sign”
One of the biggest changes in heart health is about age. Experts now have a very clear “stop sign” for people who are 60 years old or older.
If you are 60 or older and you do not have heart disease, the experts say you should not start taking a daily aspirin. As we get older, our bodies change in ways that make aspirin more dangerous.
Think of your blood vessels like an old garden hose. When a hose is new, it is strong and can handle a lot of pressure. But after sitting in the sun for years, the walls of the hose become thin and brittle. They are more likely to get tiny cracks or leaks.
In your body, these “leaks” are called internal bleeding. If you take aspirin, it makes your blood very thin. If a tiny leak starts in your stomach or your brain, the thin blood will not stop flowing. This can lead to a “hemorrhagic stroke” (a brain bleed) or a very bad stomach ulcer. These can be much worse than the heart attack you were trying to prevent.
For people between the ages of 40 and 59, it is an “individual decision.” You should only think about aspirin if your 10-year risk of heart disease is 10% or higher. This is a special score your doctor can calculate. If your risk is lower than 10%, or if you have any risk of bleeding, the experts say aspirin is likely a bad idea.
4. Takeaway #2: Why the “Baby Dose” is the Boss (81mg vs. 325mg)
In the past, some people took a full-strength “adult” aspirin (325 mg), while others took a “baby” aspirin (81 mg). A very big study called ADAPTABLE looked at over 15,000 people to see which dose was better.
The study found that the 81 mg dose worked just as well as the 325 mg dose at preventing death and heart attacks. Taking the bigger pill did not give people “extra protection.” However, the results were a little bit “messy.” This is because about 41% of the people who were supposed to take the big pill switched to the baby pill during the study. This makes it a little harder for scientists to be 100% sure, but most doctors now agree that 81 mg is the best choice.
There is also a science reason why 81 mg is better. Your body has “good” chemicals called prostacyclin that actually help protect your heart and keep your pipes open. When you take a small dose of aspirin, it stops the “bad” blood clots but leaves the “good” chemicals alone. When you take a big 325 mg dose, it “erodes selectivity.” This is a fancy way of saying it wipes out the good chemicals too. This can actually hurt your heart’s natural protection.
5. Takeaway #3: The “Memory” of a Platelet
To understand why aspirin is so powerful, you have to meet your platelets. Platelets are tiny parts of your blood that act like “sticky notes.” Their job is to rush to a cut and stick together to form a plug. This stops the bleeding and helps you heal.
Aspirin works by “breaking” the glue on the back of these sticky notes. Once a platelet touches aspirin, it can never be sticky again. Because platelets are very simple, they cannot fix themselves.
Here is the most important part: a platelet lives for about 7 to 10 days. Even though the aspirin pill leaves your body in just 20 minutes, the platelets that were “broken” will stay broken for their whole life. Your body has to grow brand-new platelets to get that “stickiness” back.
This leads to life-saving advice: If you have a surgery scheduled, you must tell your surgeon if you are taking aspirin. You usually have to stop taking it at least one full week before your surgery. If you don’t wait that 7 to 10 days, your blood won’t be able to clot during the operation, which can be very dangerous.
6. Takeaway #4: The Diabetes Tie-Breaker
People with diabetes have a higher risk of heart trouble, so many doctors used to think aspirin was a “no-brainer” for them. But a famous study called ASCEND checked to see if this was true.
The study found a strange “tie.”
- Aspirin helped prevent heart events in 1% of people.
- But aspirin caused major bleeding in 9% of people.
When you look at 1.1% versus 0.9%, the numbers are almost the same. This is called “asymmetry.” It means that for almost every person aspirin helped, it harmed another person. Because of this, even people with diabetes should not just start taking aspirin without a very deep talk with their doctor. It is no longer a simple “yes” for everyone.
7. Takeaway #5: The “Crystal Ball” Heart Scan (CAC)
Doctors are moving away from “one-size-fits-all” rules. They are now using a tool called a Coronary Artery Calcium (CAC) scan.
Think of this scan like a crystal ball. It is a quick picture that looks for hard “calcium” or plaque inside your heart pipes. This tells the doctor exactly how much disease is actually there.
A study called MESA showed us how to use these scores:
- If your score is 0: Your pipes look very clean. In this case, aspirin is almost all risk and no reward. The data shows that for people with a score of 0, you would have to treat 1,190 people to help one person, but you would end up harming 567 people with bleeding. The risk of harm is twice as high as the chance of help!
- If your score is 100 or higher: This means you have a lot of plaque. For these people, aspirin is much more likely to be helpful.
This scan helps your doctor stop guessing and start using a plan that is made just for you.
8. Takeaway #6: Better Ways to Protect Your Heart
One reason we don’t need aspirin as much today is that we have better tools. Years ago, we didn’t have great ways to fix high cholesterol or high blood pressure. Aspirin was one of the only tools we had to protect the heart.
Today, we have medicines called statins that lower cholesterol very safely. We also have better ways to manage blood pressure. These treatments are much better than aspirin at stopping heart attacks, and they do not cause the same dangerous bleeding.
Stopping smoking is also much more powerful than any aspirin pill. As we get better at using these other tools, the “job” left for aspirin gets smaller and smaller. For most healthy people, if you are already taking a statin and your blood pressure is good, adding aspirin doesn’t help you more—it just adds a risk of a stomach bleed.
9. Conclusion: The New Heart Health Conversation
The medical world has changed its mind. Aspirin is a powerful medicine that should be treated with respect. While it is still a “cornerstone” for people who have already had heart disease, it is no longer recommended for most healthy people.
If you are taking aspirin today “just in case,” it is time to have a new conversation with your doctor. You can use this “Cheat Sheet” to see where you might fit:
Aspirin Heart Health Cheat Sheet
- If you have had a heart attack, stroke, or stent: You should almost always CONTINUE your 81 mg aspirin. It is very important for you.
- If you are 60 or older and healthy: You should generally NOT START The risk of bleeding is too high.
- If you are 40 to 59 and healthy: It depends. If your 10-year risk is over 10%, talk to your doctor.
- If you have a heart scan (CAC) score of 0: You should AVOID aspirin because the risk of harm is twice as high as the benefit.
- If you have a heart scan (CAC) score of 100+: You should CONSIDER aspirin if your bleeding risk is low.
Science is helping us move away from old habits. By looking at your own specific risks, you and your doctor can decide if aspirin is a life-saving tool or a dangerous risk for you. If you’re taking it today, do you know which “group” you fall into? It might be time for a new conversation.
DEEP DIVE
Aspirin in Cardiovascular Prevention
An Evidence-Based Review of Efficacy, Safety, Dose–Response, and Patient-Specific Stratification in Primary and Secondary Prevention
| Publisher | Curing Heart Disease, LLC — curingheartdisease.com |
| Author | Peter Megdal, PhD |
| Document type | Educational evidence review (clinician- and informed-reader-facing) |
| Version | 2.2 — final (publication-ready) |
| Release date | June 23, 2026 |
| Suggested review date | June 2028, or upon revision of USPSTF / ACC-AHA aspirin guidance |
| Evidence basis | Primary peer-reviewed trials, individual-participant meta-analyses, and guideline statements published in peer-reviewed journals (JAMA, Lancet, NEJM, Circulation). Guideline anchors: USPSTF 2022; ACC/AHA Primary Prevention 2019; AHA/ACC Chronic Coronary Disease 2023; ACC/AHA Acute Coronary Syndromes 2025. |
| Disclosures | No commercial sponsorship. No industry funding. Author reports no relevant financial conflicts of interest. |
| Key safety framing — read first
• The benefit–risk balance of aspirin differs fundamentally between secondary prevention (people who already have established cardiovascular disease) and primary prevention (people who do not). Conclusions in one setting do not transfer to the other. • For primary prevention, current U.S. Preventive Services Task Force guidance recommends an individualized decision only for adults aged 40–59 with a 10-year cardiovascular risk of 10% or higher who are not at increased bleeding risk, and recommends against initiating aspirin in adults aged 60 or older. • “Do not initiate for primary prevention” is not the same as “stop aspirin” or “never use aspirin.” People taking aspirin for established disease should not discontinue it based on primary-prevention data. • This document is educational and does not constitute individual medical advice. Any decision to start, change, or stop aspirin should be made with a qualified clinician, who can weigh personal ischemic and bleeding risk. |
Contents
- Introduction and the primary–secondary prevention paradigm…………………………………………. 3
- Pharmacology and mechanism of action……………………………………………………………………….. 3
- Dose–response and dosing frequency………………………………………………………………………….. 4
- Body weight and mass-based dosing……………………………………………………………………………. 5
- Patient-specific considerations……………………………………………………………………………………… 6
- Advanced risk stratification: coronary artery calcium………………………………………………………. 7
- Family history of premature coronary disease………………………………………………………………… 7
- Complementary and alternative preventive strategies…………………………………………………….. 8
- Quantitative benefit and harm………………………………………………………………………………………. 8
- Summary of recommendations by population………………………………………………………………. 9
- Synthesis: key questions………………………………………………………………………………………….. 10
- Plain-language summary………………………………………………………………………………………….. 11
- Limitations and evidence quality……………………………………………………………………………….. 11
- Disclaimer………………………………………………………………………………………………………………. 12
References…………………………………………………………………………………………………………………… 13
1. Introduction and the primary–secondary prevention paradigm
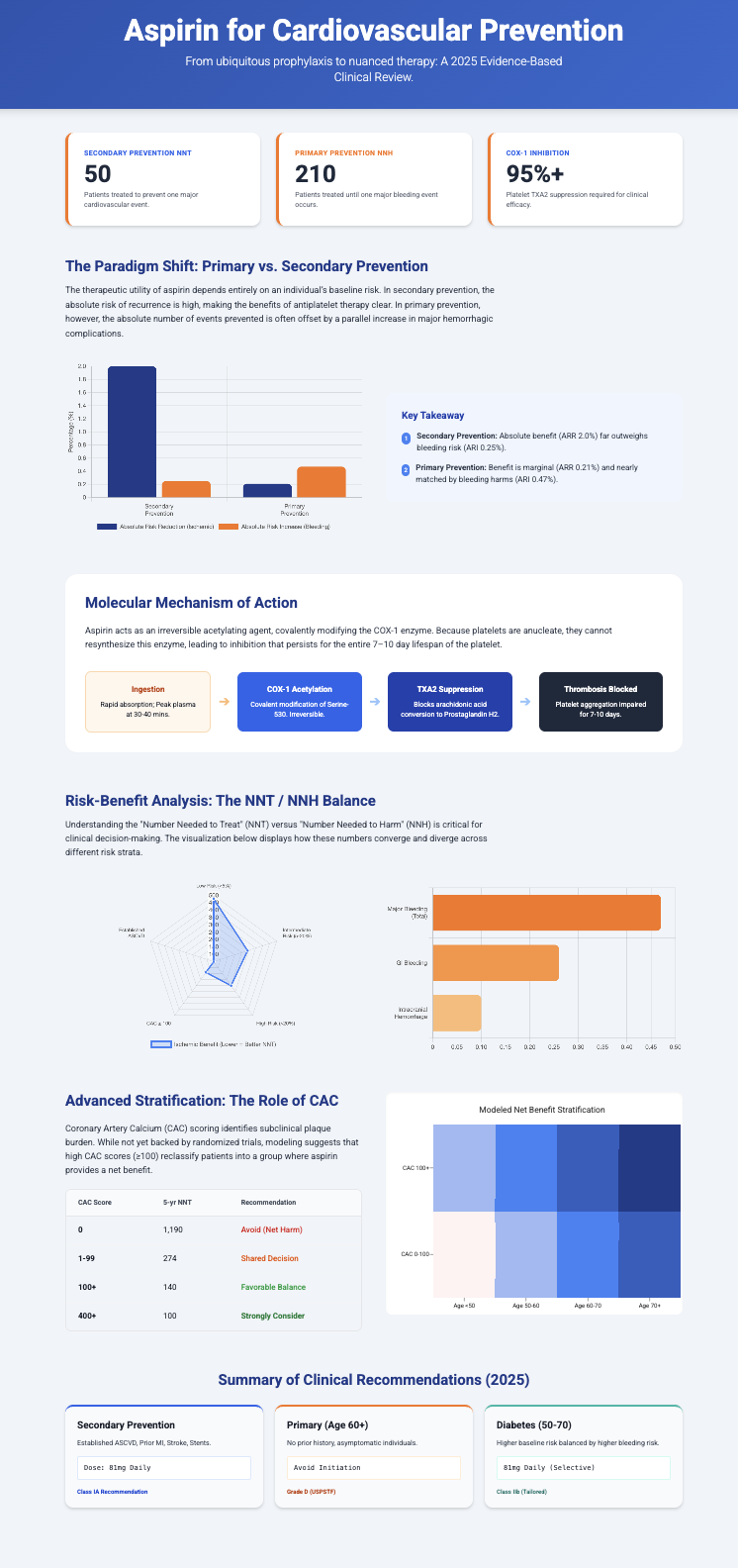
The role of acetylsalicylic acid (aspirin) in cardiovascular medicine has narrowed substantially over the past two decades. Aspirin was once recommended broadly as a daily prophylactic for adults seeking to prevent cardiovascular disease; it is now understood to have a narrow therapeutic margin that depends heavily on an individual’s baseline ischemic and bleeding risk. Because aspirin prevents occlusive arterial events through the same antiplatelet mechanism that impairs normal hemostasis, its net value rises and falls with the absolute risk of the events it is meant to prevent.[1,2]
The single most important distinction in interpreting the aspirin evidence is between two populations. Secondary prevention applies to people with documented cardiovascular disease—prior myocardial infarction, ischemic stroke or transient ischemic attack, stable or unstable angina, peripheral arterial disease, or prior revascularization (percutaneous coronary intervention or coronary artery bypass grafting). These individuals carry a high absolute risk of recurrent thrombotic events, so even a moderate relative risk reduction produces a large absolute benefit that clearly outweighs bleeding hazard. [2]
Primary prevention applies to people without clinically evident cardiovascular disease. Their absolute annual event rate is low, so the absolute number of ischemic events prevented is small and is largely offset by a parallel absolute increase in major bleeding, principally gastrointestinal hemorrhage and intracranial hemorrhage. This asymmetry—similar relative effects but very different absolute effects—is the central reason contemporary guidance has moved away from routine primary-prevention use. [2,1]
In the landmark individual-participant meta-analysis of the Antithrombotic Trialists’ (ATT) Collaboration, the proportional reduction in serious vascular events was broadly similar in the two settings, but the absolute effects diverged sharply: about a 0.06% per-year absolute reduction in primary prevention versus an absolute reduction roughly an order of magnitude larger in secondary prevention. [2]
Three modern primary-prevention trials reported in 2018 reinforced this picture in a contemporary treatment era. ARRIVE randomized 12,546 patients judged to be at moderate cardiovascular risk (and without diabetes or high bleeding risk) to 100 mg of aspirin or placebo; it found no significant reduction in the primary composite cardiovascular endpoint, with more gastrointestinal bleeding (mostly mild to moderate) and no difference in fatal events. Notably, the observed event rate was far lower than projected (roughly 9% versus an anticipated 17%), so the cohort effectively behaved like a lower-risk population—partly because many participants were already taking statins and antihypertensives. [16]
ARRIVE’s companions completed the contemporary trio: ASCEND tested aspirin in diabetes and ASPREE in older adults (both detailed in Section 5). Together, these trials are the empirical basis for the shift away from routine primary-prevention aspirin. [8,5]
2. Pharmacology and mechanism of action
Aspirin’s antithrombotic effect derives from irreversible inhibition of platelet cyclooxygenase-1 (COX-1). Aspirin acetylates a serine residue (Ser-530) within the COX-1 catalytic channel, sterically blocking arachidonic acid from reaching the active site and permanently halting synthesis of the downstream prostanoid thromboxane A₂ (TxA₂), a potent promoter of platelet activation, aggregation, and vasoconstriction. [3,4]
Because platelets are anucleate and cannot synthesize new protein, COX-1 blockade persists for the platelet’s entire lifespan of roughly 7–10 days. This durable antiplatelet effect contrasts with aspirin’s brief pharmacokinetic exposure: peak plasma concentration occurs within about 30–40 minutes and the plasma half-life is only about 15–20 minutes owing to rapid esterase hydrolysis to salicylate. Even transient portal and systemic exposure is sufficient to inactivate the circulating platelet pool. [3,4]
Vascular endothelial cells, by contrast, are nucleated and can resynthesize cyclooxygenase. They produce prostacyclin (PGI₂), a vasodilator and platelet inhibitor that physiologically opposes TxA₂. Low daily doses (about 75–100 mg) achieve near-complete platelet COX-1 inhibition while relatively sparing endothelial prostacyclin, in part because platelets are exposed to aspirin in the portal circulation before first-pass hepatic metabolism. Higher daily doses progressively suppress endothelial prostacyclin as well, eroding this selectivity without adding antithrombotic benefit. [3,4]
This dual influence defines aspirin’s benefit–risk profile. Suppressing platelet aggregation reduces shear-induced arterial thrombosis at sites of plaque rupture, but the same impairment of hemostasis raises the risk of mucosal, gastrointestinal, and intracranial bleeding. [2,3]
3. Dose–response and dosing frequency
Pharmacodynamic studies show that platelet TxA₂ synthesis is nearly fully suppressed by daily doses in the 75–100 mg range, and that antiplatelet efficacy reaches a plateau above this range. Higher maintenance doses (for example 162–325 mg) have not shown added antithrombotic benefit in long-term prevention, and they are associated with greater dose-dependent gastrointestinal mucosal injury in pharmacologic and historical studies—though, as noted below, the randomized ADAPTABLE comparison did not itself detect a statistically significant difference in major bleeding. Single immediate-release loading doses of 162–325 mg are used in acute coronary syndromes and acute ischemic stroke to achieve rapid platelet inhibition; this is a distinct, acute indication. [3,4,23]
The clearest contemporary evidence on maintenance dose comes from the ADAPTABLE pragmatic trial, which randomized 15,076 patients with established atherosclerotic cardiovascular disease to 81 mg or 325 mg of aspirin daily. Over a median 26.2 months, the primary effectiveness outcome (a composite of all-cause death, hospitalization for myocardial infarction, or hospitalization for stroke) did not differ significantly (estimated event rates 7.28% for 81 mg versus 7.51% for 325 mg; hazard ratio 1.02, 95% CI 0.91–1.14), nor did hospitalization for major bleeding (HR 1.18, 95% CI 0.79–1.77). [9]
These results should be read as “no significant difference was detected,” not as proof of exact equivalence. ADAPTABLE was open-label and had substantial crossover: roughly 41% of patients assigned to 325 mg switched to 81 mg, while only about 7% switched in the other direction. Such asymmetric crossover biases the comparison toward the null and limits how strongly a true dose difference can be excluded. With that caveat, the trial supports 81 mg daily as the preferred maintenance dose for most patients on the basis of comparable measured outcomes and better tolerability and adherence. Contemporary guidance is concordant: the 2023 AHA/ACC Chronic Coronary Disease guideline recommends low-dose aspirin (75–100 mg, commonly 81 mg) as a Class 1 (Level of Evidence A) single-antiplatelet strategy for patients with chronic coronary disease not on oral anticoagulation. [9,21]
Consistent with this, the CURRENT-OASIS 7 program in acute coronary syndromes found that continued higher-dose (300–325 mg) aspirin was not superior to lower-dose (75–100 mg) aspirin for major ischemic outcomes and was associated with more minor and gastrointestinal bleeding—reasoning echoed in the 2025 ACC/AHA acute coronary syndromes guideline, which endorses 75–100 mg for maintenance therapy. [10,22]
3.1 Dosing frequency and platelet turnover
Dosing interval is constrained by platelet turnover. The marrow releases a fraction of new, uninhibited platelets into the circulation each day, so once-daily dosing is required to maintain steady-state inhibition. Alternate-day dosing leaves “off-day” gaps during which newly formed platelets restore thromboxane capacity. In the Women’s Health Study, 100 mg of aspirin every other day did not significantly reduce the primary composite of major cardiovascular events in initially healthy women over roughly 10 years, although it reduced ischemic stroke. [15]
Pharmacodynamic work helps explain that result: 100 mg taken every other day produces less and more variable platelet inhibition than 81 mg taken daily, suggesting the alternate-day regimen may have under-dosed participants on off days. This reduced platelet suppression may partially explain the Women’s Health Study findings, although alternative explanations—lower-than-expected event rates, limited statistical power, and trial-design differences—may also contribute. By similar logic, extending the interval further (every third day) is not supported by clinical-endpoint evidence and is not recommended. [18,19,23]
Conversely, in conditions with accelerated platelet turnover—such as essential thrombocythemia and some patients with type 2 diabetes—once-daily dosing can leave incomplete inhibition before the next dose. Pharmacodynamic studies indicate that twice-daily low-dose aspirin can restore more consistent thromboxane suppression in these settings than simply increasing the once-daily dose; this remains a specialized strategy rather than general practice. [4]
4. Body weight and mass-based dosing
Whether a fixed low dose suits all body sizes is unsettled. In a pooled individual-participant analysis of more than 100,000 participants across primary- and secondary-prevention trials, Rothwell and colleagues reported a dose–weight interaction: low-dose aspirin (75–100 mg) reduced cardiovascular events mainly in people weighing under about 70 kg, with little benefit above that weight, whereas higher doses (≥325 mg) were effective mainly at higher body weight. The analysis also signaled potential harm at the extremes—greater case fatality of a first cardiovascular event in heavier people taking low-dose aspirin, and increased all-cause mortality among people under 50 kg (hazard ratio 1.52, 95% CI 1.04–2.21). [11]
These findings are hypothesis-generating, not practice-defining, and have not been confirmed prospectively. In a prespecified analysis of ASPREE in older adults, body weight did not modify aspirin’s cardiovascular effect, and bleeding risk was not lower in heavier individuals. Pharmacodynamic studies in adults without diabetes have likewise found platelet inhibition by 81 mg or 325 mg to be largely independent of body mass. Subsequent analyses have not consistently replicated the body-weight interaction, and no major guideline currently recommends weight-adjusted aspirin dosing; the most reasonable current reading is that weight-tailored dosing is intriguing but not clinically actionable. [5,11]
5. Patient-specific considerations
5.1 Age
Bleeding risk rises steeply with age, while the absolute ischemic benefit of primary-prevention aspirin remains modest. The ASPREE trial randomized 19,114 community-dwelling adults (largely aged 70 and older) to 100 mg daily or placebo. Aspirin did not prolong disability-free survival (HR 1.01, 95% CI 0.92–1.11) and did not significantly reduce cardiovascular disease (10.7 versus 11.3 events per 1,000 person-years; HR 0.95, 95% CI 0.83–1.08), but it significantly increased major hemorrhage (8.6 versus 6.2 events per 1,000 person-years; HR 1.38, 95% CI 1.18–1.62) and was associated with higher all-cause mortality (HR 1.14, 95% CI 1.01–1.29), largely cancer-related and interpreted cautiously by the investigators. [5,6,7]
These data underpin current guidance: in primary prevention, an individualized decision is reasonable only for adults aged 40–59 at sufficiently high cardiovascular risk and low bleeding risk, and initiation is not recommended at age 60 or older. The USPSTF additionally suggests considering discontinuation of primary-prevention aspirin around age 75. None of this applies to secondary prevention. [1]
5.2 Biological sex
Earlier sex-specific analyses suggested aspirin’s primary-prevention benefit was driven more by stroke reduction in women and myocardial-infarction reduction in men. Subsequent work indicates much of this apparent difference may reflect body-size and pharmacokinetic factors rather than sex-specific biology, and contemporary guidance does not recommend different aspirin strategies by sex in primary prevention. [2,11]
5.3 Diabetes mellitus
People with diabetes are at elevated cardiovascular risk, but they also bleed more. The ASCEND trial randomized 15,480 adults with diabetes and no known cardiovascular disease to 100 mg daily or placebo. Over a mean 7.4 years, aspirin reduced serious vascular events (8.5% versus 9.6%; rate ratio 0.88, 95% CI 0.79–0.97) but increased major bleeding (4.1% versus 3.2%; rate ratio 1.29, 95% CI 1.09–1.52). The absolute benefit (about 1.1%) was closely matched by the absolute bleeding excess (about 0.9%), corresponding to roughly 91 treated to prevent one serious vascular event and roughly 112 treated to cause one major bleed; no subgroup showed benefit clearly exceeding harm. Aspirin in diabetes therefore requires individualized, shared decision-making rather than routine use. [8]
5.4 Concomitant risk factors
Active smoking and uncontrolled hypertension raise both atherosclerotic risk and bleeding risk (including intracranial hemorrhage). Because risk factors for ischemic events overlap heavily with risk factors for bleeding, raising baseline cardiovascular risk does not automatically tip the balance toward net benefit. Aggressive control of blood pressure and tobacco use is both a safer and a more effective first priority than initiating aspirin. [2,17]
6. Advanced risk stratification: coronary artery calcium
Because population risk equations imperfectly identify who will actually benefit, coronary artery calcium (CAC) scoring has been studied as a tool to allocate primary-prevention aspirin to those most likely to gain. In analyses of the Multi-Ethnic Study of Atherosclerosis (MESA), restricted to aspirin-naïve adults under 70 not at high bleeding risk, the relationship between the 5-year number-needed-to-treat (NNT₅) and number-needed-to-harm (NNH₅) shifted favorably as CAC rose. Overall the NNT₅ (476) exceeded the NNH₅ (355); for CAC ≥100 the NNT₅ (140) fell below the NNH₅ (518), indicating a modeled net benefit; and for CAC = 0 the NNT₅ (1,190) far exceeded the NNH₅ (567), indicating a modeled net harm. [12,13]
These are modeled estimates derived from observational data, not results from randomized allocation of aspirin by CAC. The 2019 ACC/AHA primary-prevention guideline treats CAC as a risk-enhancing tool to refine risk assessment rather than as a validated test for selecting aspirin therapy; no randomized trial has yet shown that allocating aspirin by CAC improves outcomes. The estimates below should therefore inform shared decision-making, not replace it. [17,12]
Table 1. CAC-guided modeled estimates of aspirin benefit versus harm in primary prevention (MESA; aspirin-naïve adults <70 years, not at high bleeding risk). Modeling assumed a 12% relative reduction in CVD events and a 42% relative increase in major bleeding; figures are observational estimates, not randomized evidence. NNT₅/NNH₅ = 5-year number needed to treat / to harm.
| CAC stratum | 5-year NNT₅ (prevent 1 CVD event) | 5-year NNH₅ (cause 1 major bleed) | Modeled net effect |
| Overall cohort | 476 | 355 | Modeled harm ≥ benefit |
| CAC = 0 | 1,190 | 567 | Modeled net harm — avoid |
| CAC ≥ 100 | 140 | 518 | Modeled net benefit (no RCT) |
CAC therefore offers a more personalized basis for refining risk than scores alone: a score of zero identifies people in whom bleeding risk likely dominates, while a high score identifies subclinical plaque burden in which aspirin may be biologically justified, provided bleeding risk is low. These remain modeled inferences pending randomized confirmation. An ultrasound-based carotid plaque score has been studied for the same purpose, with the presence of carotid plaque at higher estimated ASCVD risk marking a more favorable balance. [20]
7. Family history of premature coronary disease
A family history of premature coronary artery disease (a first-degree male relative affected before 55 or female relative before 65) is recognized in the 2019 ACC/AHA primary-prevention guideline as a risk-enhancing factor that can refine risk assessment. It can meaningfully reclassify an individual’s estimated risk upward, and a strong family history may appropriately prompt further assessment—such as CAC testing—to clarify whether preventive intensification is warranted. It is not, however, an established stand-alone indication for primary-prevention aspirin, and it does not reduce aspirin’s bleeding hazard. The appropriate response to a strong family history is intensified guideline-directed prevention—lipid management, blood-pressure control, and lifestyle measures—rather than reflexive aspirin initiation. [17,1]
8. Complementary and alternative preventive strategies
In the modern primary-prevention era, several interventions offer a more favorable benefit–risk profile than aspirin. Statin therapy substantially reduces major cardiovascular events without increasing major hemorrhage, and serious adverse effects such as rhabdomyolysis are rare. Strict blood-pressure control reduces stroke and myocardial infarction without raising bleeding risk—and directly lowers the risk of hemorrhagic stroke. Smoking cessation produces large, rapid reductions in cardiovascular risk. [17]
These alternatives also reshape the case for aspirin itself. As background statin use and risk-factor control reduce residual ischemic risk, the incremental absolute benefit of adding aspirin in primary prevention shrinks while its bleeding risk persists. For most people without established disease who are already on guideline-directed therapy, adding aspirin offers little net advantage. [2,17]
9. Quantitative benefit and harm
The tables below summarize effect estimates from the principal peer-reviewed sources. Relative effects are broadly similar across settings; the decisive difference is in absolute effect, which is governed by baseline risk. All figures are drawn directly from the cited trials and meta-analyses.
Table 2. Aspirin effects by prevention setting and population, from primary peer-reviewed sources. RR = rate/relative ratio; HR = hazard ratio; CI = confidence interval.
| Setting / population | Effect (95% CI) | Outcome and absolute effect | Source |
| Primary prevention — serious vascular events | RR 0.88 (0.82–0.94) | 0.51% vs 0.57% per year; ≈12% proportional reduction | ATT meta-analysis |
| Primary prevention — major coronary events | RR 0.82 (0.75–0.90) | ≈18% proportional reduction | ATT meta-analysis |
| Primary prevention — stroke (total) | RR 0.95 (0.85–1.06) | No significant effect | ATT meta-analysis |
| Primary prevention — major extracranial bleeding | RR 1.54 (1.30–1.82) | 0.10% vs 0.07% per year; significant increase | ATT meta-analysis |
| Primary prevention in diabetes — serious vascular events | RR 0.88 (0.79–0.97) | 8.5% vs 9.6%; ARR ≈1.1%; NNT ≈91 | ASCEND |
| Primary prevention in diabetes — major bleeding | RR 1.29 (1.09–1.52) | 4.1% vs 3.2%; ARI ≈0.9%; NNH ≈112 | ASCEND |
| Primary prevention in older adults — CVD | HR 0.95 (0.83–1.08) | 10.7 vs 11.3 / 1,000 py; not significant | ASPREE |
| Primary prevention in older adults — major hemorrhage | HR 1.38 (1.18–1.62) | 8.6 vs 6.2 / 1,000 py; significant increase | ASPREE |
| Secondary prevention — serious vascular events | ≈one-fifth proportional reduction | ≈6.7% vs 8.2% per year; large absolute benefit | ATT meta-analysis |
Table 3. Maintenance-dose comparison (81 mg vs 325 mg daily) in secondary prevention.
| Outcome | 81 mg | 325 mg | Effect (95% CI) |
| Composite: death, MI, or stroke hospitalization | 7.28% | 7.51% | HR 1.02 (0.91–1.14) |
| Hospitalization for major bleeding | — | — | HR 1.18 (0.79–1.77) |
| Switched to the other dose (crossover) | ≈7% | ≈41% | Asymmetric — biases toward null |
Source: ADAPTABLE. The marked asymmetric crossover is the key limitation and is why the trial supports 81 mg as preferred without proving exact dose equivalence. [9]
10. Summary of recommendations by population
The table below states, for each population, the action (initiate, continue, or avoid) together with its setting and the supporting guidance. Every row preserves the primary-versus-secondary distinction.
| Population | Action | Rationale | Guidance |
| Established ASCVD / post-MI / post-stroke / post-PCI or CABG (secondary prevention) | Continue (81 mg daily) | High recurrent-event risk; absolute benefit far exceeds bleeding risk | 2023 AHA/ACC CCD (Class 1, LOE A); ATT; ADAPTABLE |
| Primary prevention, age 40–59, 10-yr CVD risk ≥10%, low bleeding risk | Individualize | Small net benefit; depends on personal risk and preference | USPSTF Grade C |
| Primary prevention, age ≥60 | Do not initiate | No net benefit; bleeding risk dominates | USPSTF Grade D |
| Primary prevention with elevated bleeding risk (any age) | Do not initiate | Bleeding hazard outweighs any ischemic benefit | USPSTF; ACC/AHA |
| Primary prevention, CAC = 0 | Avoid | Modeled net harm; very low ischemic risk (observational estimate) | MESA modeling |
| Primary prevention, CAC ≥100, low bleeding risk | Consider | Modeled net benefit (NNT₅ < NNH₅); no randomized confirmation | MESA modeling |
| Primary prevention in diabetes, no ASCVD | Individualize | Benefit and bleeding excess closely matched | ASCEND; ADA/guidelines |
11. Synthesis: key questions
Who benefits most?
People with established cardiovascular disease (secondary prevention). Their high recurrent-event risk means the absolute benefit of low-dose aspirin clearly exceeds bleeding risk. Low-dose aspirin (81 mg daily) is standard long-term therapy for most secondary-prevention patients unless contraindicated or superseded by an alternative antithrombotic strategy—for example, oral anticoagulation for another indication, or a defined dual-antiplatelet course after recent stenting or acute coronary syndrome. [2,9,21]
Who benefits least?
Adults without cardiovascular disease who are already on guideline-directed prevention (effective statin therapy, blood-pressure control, non-smoking). Their residual ischemic risk is low, so added aspirin offers little incremental benefit while bleeding risk remains. [2,17]
Which populations should generally avoid initiating primary-prevention aspirin?
Adults aged 60 or older; adults of any age at increased bleeding risk; people with CAC of zero; and, on current evidence, those at the low end of body weight in whom harm signals have been raised. [1,12,11]
What is the lowest effective maintenance dose?
A daily dose of about 75–81 mg provides near-maximal platelet inhibition and comparable clinical protection to higher doses, with less gastrointestinal and bleeding toxicity. [3,9]
Is daily dosing better than alternate-day dosing?
Yes. Daily low-dose aspirin gives more consistent platelet inhibition than alternate-day dosing, because newly formed platelets restore thromboxane capacity during off-day intervals. [15,18]
Do doses above ~100 mg add cardiovascular benefit?
No consistent evidence demonstrates superior cardiovascular outcomes with routine maintenance doses above roughly 100 mg, while higher doses are associated with greater gastrointestinal toxicity. Higher single doses remain appropriate only for acute loading in acute coronary syndromes or acute stroke. [9,10,22]
What is the overall 2025-and-beyond consensus?
For secondary prevention, low-dose aspirin remains a cornerstone: the 2023 AHA/ACC Chronic Coronary Disease guideline gives low-dose aspirin (75–100 mg) a Class 1 recommendation as single-antiplatelet therapy in patients not on anticoagulation, and the 2025 ACC/AHA acute coronary syndromes guideline likewise endorses 75–100 mg maintenance dosing. For primary prevention, routine use has been abandoned; any decision should be individualized, generally limited to adults 40–59 at ≥10% 10-year risk with low bleeding risk, and is well suited to refinement with imaging-based risk markers such as CAC. [1,21,22]
12. Plain-language summary
Aspirin makes platelets—the blood cells that form clots—less able to stick together, which lowers the chance of a clot blocking an artery and causing a heart attack or stroke. Because platelets cannot repair themselves, one low dose keeps working for about 7–10 days. The same effect makes bleeding harder to stop, which is why aspirin can cause bleeding in the stomach, intestines, or brain.
The key idea is that aspirin’s value depends on whether you already have heart or vascular disease:
- If you have already had a heart attack, stroke, stent, or bypass (secondary prevention), the chance of another event is high, and daily low-dose aspirin clearly does more good than harm. Do not stop it on your own.
- If you have no history of heart or vascular disease (primary prevention), the benefit is much smaller and is largely cancelled out by bleeding risk. Guidelines advise against starting aspirin at age 60 or older, and only individualized consideration for adults 40–59 at higher risk.
Tools such as a coronary calcium scan can help identify who in the primary-prevention group might still benefit. For preventing a first heart attack or stroke, statins and blood-pressure control generally provide greater and safer protection than aspirin.
Table 4. Plain-language summary of who benefits and who should be cautious.
| Aspirin generally helps | Aspirin is usually not advised (for prevention) |
| Prior heart attack | Starting aspirin at age 60 or older |
| Prior ischemic stroke or TIA | Increased bleeding risk (ulcers, anticoagulants, etc.) |
| Coronary stent or bypass surgery | No heart disease and a coronary calcium score of zero |
| High plaque burden (CAC ≥100) with low bleeding risk | Already well-protected on statin, blood-pressure control, non-smoking |
Preferred maintenance dose when aspirin is indicated: 81 mg once daily.
13. Limitations and evidence quality
The primary-prevention estimates rest on trials conducted across different eras and risk profiles; contemporary background therapy (statins, better blood-pressure control) tends to reduce the residual benefit of aspirin relative to older trials. The dose-comparison evidence (ADAPTABLE) is open-label with substantial crossover, so it constrains rather than proves dose equivalence. Weight-based dosing and twice-daily strategies are supported mainly by pharmacodynamic and post-hoc data and have not been validated in dedicated outcome trials. CAC-based allocation rests on observational modeling rather than randomized allocation. These limitations argue for individualized, clinician-guided decisions rather than blanket rules. [9,11,12]
14. Disclaimer
This document is provided for educational and informational purposes only and does not constitute medical advice, diagnosis, or treatment, nor does it establish a clinician–patient relationship. Individual ischemic and bleeding risks, medications, and comorbidities vary widely. Any decision to start, continue, change, or stop aspirin should be made together with a qualified healthcare professional.
References
- US Preventive Services Task Force, Davidson KW, Barry MJ, et al. Aspirin Use to Prevent Cardiovascular Disease: US Preventive Services Task Force Recommendation Statement. JAMA. 2022;327(16):1577-1584. doi:10.1001/jama.2022.4983
- Antithrombotic Trialists’ (ATT) Collaboration, Baigent C, Blackwell L, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373(9678):1849-1860. doi:10.1016/S0140-6736(09)60503-1
- Awtry EH, Loscalzo J. Aspirin. Circulation. 2000;101(10):1206-1218. doi:10.1161/01.cir.101.10.1206
- Patrono C, García Rodríguez LA, Landolfi R, Baigent C. Low-dose aspirin for the prevention of atherothrombosis. N Engl J Med. 2005;353(22):2373-2383. doi:10.1056/NEJMra052717
- McNeil JJ, Wolfe R, Woods RL, et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly. N Engl J Med. 2018;379(16):1509-1518. doi:10.1056/NEJMoa1805819
- McNeil JJ, Woods RL, Nelson MR, et al. Effect of Aspirin on Disability-free Survival in the Healthy Elderly. N Engl J Med. 2018;379(16):1499-1508. doi:10.1056/NEJMoa1800722
- McNeil JJ, Nelson MR, Woods RL, et al. Effect of Aspirin on All-Cause Mortality in the Healthy Elderly. N Engl J Med. 2018;379(16):1519-1528. doi:10.1056/NEJMoa1803955
- ASCEND Study Collaborative Group, Bowman L, Mafham M, et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N Engl J Med. 2018;379(16):1529-1539. doi:10.1056/NEJMoa1804988
- Jones WS, Mulder H, Wruck LM, et al. Comparative Effectiveness of Aspirin Dosing in Cardiovascular Disease. N Engl J Med. 2021;384(21):1981-1990. doi:10.1056/NEJMoa2102137
- CURRENT-OASIS 7 Investigators, Mehta SR, Bassand JP, et al. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes. N Engl J Med. 2010;363(10):930-942. doi:10.1056/NEJMoa0909475
- Rothwell PM, Cook NR, Gaziano JM, et al. Effects of aspirin on risks of vascular events and cancer according to bodyweight and dose: analysis of individual patient data from randomised trials. Lancet. 2018;392(10145):387-399. doi:10.1016/S0140-6736(18)31133-4
- Cainzos-Achirica M, Miedema MD, McEvoy JW, et al. Coronary Artery Calcium for Personalized Allocation of Aspirin in Primary Prevention of Cardiovascular Disease in 2019: The MESA Study (Multi-Ethnic Study of Atherosclerosis). Circulation. 2020;141(19):1541-1553. doi:10.1161/CIRCULATIONAHA.119.045010
- Miedema MD, Duprez DA, Misialek JR, et al. Use of coronary artery calcium testing to guide aspirin utilization for primary prevention: estimates from the multi-ethnic study of atherosclerosis. Circ Cardiovasc Qual Outcomes. 2014;7(3):453-460. doi:10.1161/CIRCOUTCOMES.113.000690
- Steering Committee of the Physicians’ Health Study Research Group. Final report on the aspirin component of the ongoing Physicians’ Health Study. N Engl J Med. 1989;321(3):129-135. doi:10.1056/NEJM198907203210301
- Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352(13):1293-1304. doi:10.1056/NEJMoa050613
- Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018;392(10152):1036-1046. doi:10.1016/S0140-6736(18)31924-X
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596-e646. doi:10.1161/CIR.0000000000000678
- Swaim L, Hillman RS. Aspirin administered to women at 100 mg every other day produces less platelet inhibition than aspirin administered at 81 mg per day: implications for interpreting the women’s health study. J Thromb Thrombolysis. 2009;28(1):94-100. doi:10.1007/s11239-008-0262-6
- Feldman M, Cryer B, Rushin K, Betancourt J. A comparison of every-third-day versus daily low-dose aspirin therapy on serum thromboxane concentrations in healthy men and women. Clin Appl Thromb Hemost. 2001;7(1):53-57. doi:10.1177/107602960100700111
- Dzaye O, Razavi AC, Dardari ZA, et al. Carotid Ultrasound-Based Plaque Score for the Allocation of Aspirin for the Primary Prevention of Cardiovascular Disease Events: The Multi-Ethnic Study of Atherosclerosis and the Atherosclerosis Risk in Communities Study. J Am Heart Assoc. 2024;13(12):e034718. doi:10.1161/JAHA.123.034718
- Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148(9):e9-e119. doi:10.1161/CIR.0000000000001168
- Rao SV, O’Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2025;151(13):e771-e862. doi:10.1161/CIR.0000000000001309
- Patrono C. The Multifaceted Clinical Readouts of Platelet Inhibition by Low-Dose Aspirin. J Am Coll Cardiol. 2015;66(1):74-85. doi:10.1016/j.jacc.2015.05.012