I. Executive Summary: The Necessity of Training Modification
The management of Atrial Fibrillation (Afib) in the Masters athlete (defined generally as age 35 and above, and specifically in this context as 50+) presents a critical challenge that necessitates a nuanced shift in training philosophy. While chronic endurance training offers broad cardiovascular benefits, it is fundamentally a dose-dependent risk factor for atrial arrhythmias. For an athlete who has undergone treatment (ablation or pharmacological therapy) for Afib, continuing intense, high-volume training carries a substantial probability of arrhythmia recurrence and disease progression.
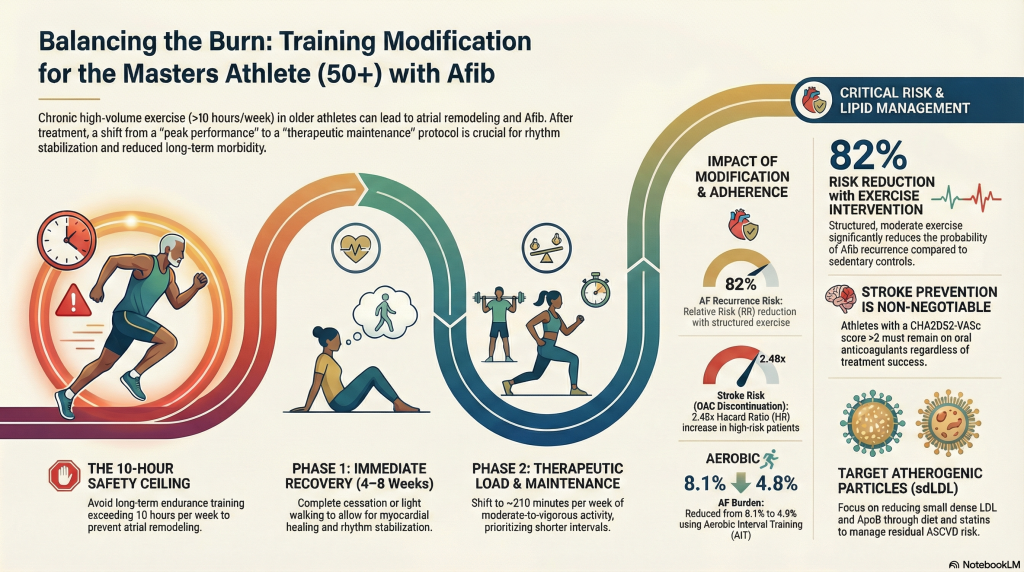
The primary conclusion supported by electrophysiology research is that the Masters athlete (50+) diagnosed and treated for Afib should immediately and significantly moderate the volume and intensity of endurance training. This reduction is required not merely for symptomatic relief but as a therapeutic strategy to stabilize the atrial substrate and reduce long-term morbidity. The goal should be to maintain high cardiovascular fitness through structured, moderate-to-vigorous activity, while actively mitigating the structural and electrical strain associated with peak endurance performance.
Key Pillars for Clinical Management:
- Training Dose Adjustment: Shift training volume away from chronic, high-intensity endurance training (typically defined as >10 hours per week over many years 1).
- Rhythm Stability and Recurrence Risk: Implement therapeutic exercise protocols, such as Aerobic Interval Training (AIT), which have been shown to actively reduce Afib burden.2
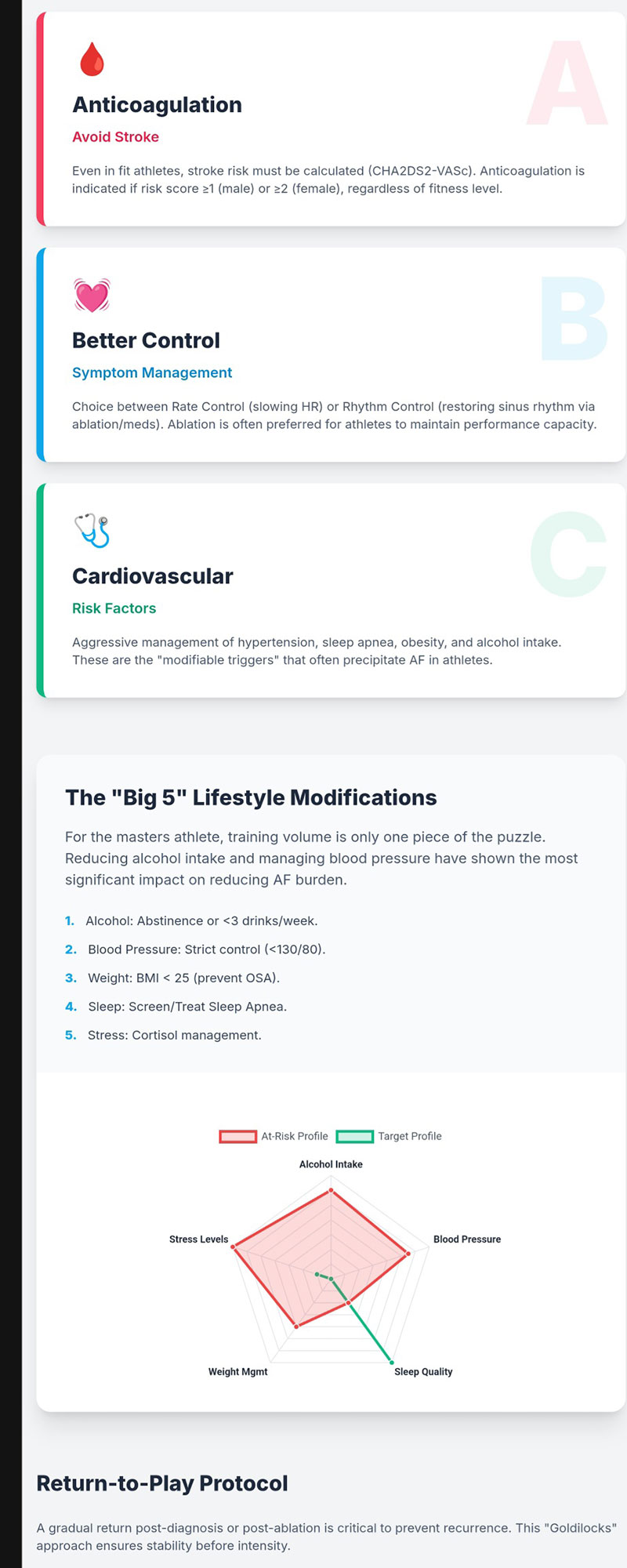
- Stroke Prevention: Adherence to Oral Anticoagulation (OAC) guidelines based on individual risk scores (e.g., CHA2DS2-VASc) is critical and often outweighs athletic goals, as successful ablation does not universally guarantee safety from stroke.4
II. Pathophysiology and Statistical Probability of Afib Recurrence
A. The Causal Mechanism: Endurance Training and Atrial Remodeling
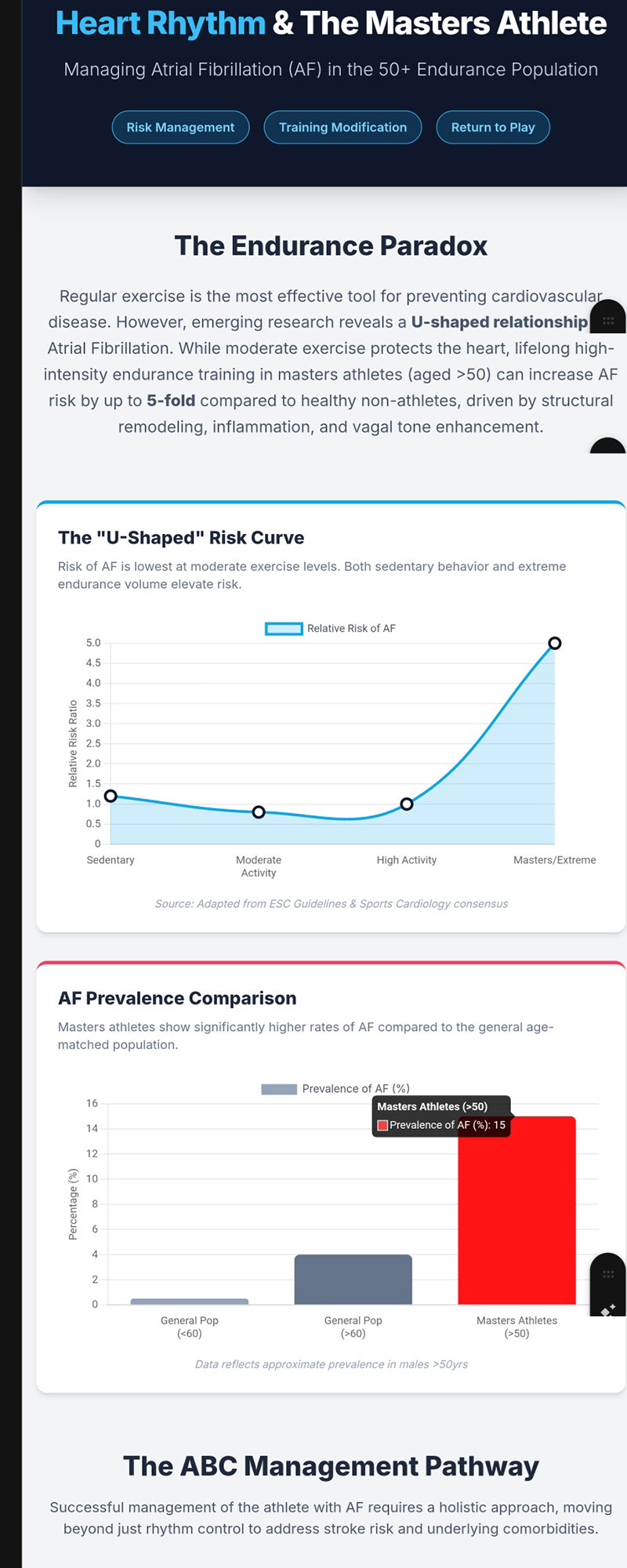
The risk of Afib in Masters athletes is inextricably linked to the physiological adaptations induced by sustained, high-volume training, often summarized by the J- or U-shaped curve model of exercise dose and cardiovascular risk.5
Cardiac Structural and Electrical Substrate
Chronic volume loading inherent to endurance sports (such as cycling, running, or swimming) results in specific cardiac remodeling, leading to the “athlete’s heart”.7 While much attention is paid to ventricular changes, it is the atrial remodeling that predisposes the athlete to Afib. This remodeling includes:
- Biatrial Dilation: Enlargement of both the left and right atria.7
- Myocardial Fibrosis: The development of microscopic scarring (fibrosis) within the atrial walls.8
This fibrosis is particularly dangerous because it creates an electrically heterogeneous tissue environment, providing a substrate highly conducive to the formation of macro-reentry electrical circuits. These circuits sustain the disorganized electrical activity characteristic of Afib.8
Autonomic Imbalances as Triggers
In addition to structural changes, endurance athletes experience profound fluctuations in their autonomic nervous system. They typically exhibit exaggerated vagal tone at rest, leading to sinus bradycardia. However, intense or competitive exercise induces a powerful sympathetic surge. This swing in autonomic activity significantly shortens the atrial refractory period, acting as a potent ectopic trigger that can initiate Afib episodes.8 In the Masters athlete (50+), the combination of exercise-induced remodeling and age-related risk factors (such as hypertension or obesity, even if well-controlled) compounds this electrophysiological vulnerability.1
B. Statistical Data on Recurrence Probability Post-Treatment
The probability of remaining free from atrial arrhythmia after treatment is notably challenged by the continuation of the underlying etiological stimulus (intense training).
Recurrence Post-Catheter Ablation (PVI)
For athletes undergoing catheter ablation, specifically Pulmonary Vein Isolation (PVI), the recurrence rates are often problematic. Observational data suggest that endurance athletes tend to experience higher rates of atrial arrhythmia recurrence than sedentary non-athletes after the procedure.10 Crucially, this recurrence often manifests not as the original Afib, but as atypical flutter.10 This phenomenon suggests that the disease process has progressed, with the original pulmonary vein triggers successfully isolated, but the underlying fibrotic substrate driving new arrhythmias elsewhere in the atrial tissue (non-pulmonary vein dependent).10
One study comparing PVI outcomes reported that athletes experienced similar arrhythmia-free survival at 3 years compared to non-endurance controls (87% vs. 85%, p=0.88).9 However, another comparison showed recurrence rates (freedom from AF and antiarrhythmic therapy) were 34% in athletes versus 48% in controls after 3 years.9 The implication of this variation is that while PVI may be effective initially for vagally-mediated Afib common in athletes, the long-term maintenance of intense training will relentlessly drive further remodeling and increase the probability of eventual recurrence or progression to more complex arrhythmias like atrial flutter.10
Quantitative Benefit of Training Modification
A structured reduction and modification of exercise volume are strongly supported by outcome data, translating to a favorable reduction in recurrence probability.
- Relative Risk Reduction: Structured exercise intervention has been associated with an overall reduced risk of AF recurrence compared to control groups, quantified by a Relative Risk (RR) of 82 (95% CI: 0.68 to 0.99, p=0.04).3 This reduction suggests that thoughtful exercise prescription, focused on health maintenance rather than maximum performance, can be genuinely therapeutic.
- Reduction in Afib Burden: Specifically, structured Aerobic Interval Training (AIT) was found to reduce the mean time an athlete spent in Afib from 1% to 4.8% compared to a control group, alongside improvements in cardiopulmonary fitness (V02max).2
C. The Unacceptable Risk of Stroke
The decision to continue intense training must be weighed against the persistent risk of stroke, particularly because the athlete is over 50 years of age. Age 50+ likely results in a CHA2DS2-VASc score of at least 1 (for age), possibly 2 or higher if other risk factors like hypertension or diabetes are present.4
Stroke prevention guidelines dictate the use of Oral Anticoagulation (OAC) based on the CHA2DS2-VASc score, regardless of the perceived success of Afib treatment.
- OAC Discontinuation Risk: Observational studies indicate that for patients with a CHA2DS2-VASc score > 2, discontinuing OAC >3 months after catheter ablation led to a substantially increased stroke risk, quantified by a Hazard Ratio (HR) of 2.48 (95% CI, 1.11–5.52; P<0.05).4
- Ablation Limitations: Randomized clinical trials have, to date, not demonstrated reductions in stroke risk after catheter ablation.4
This data underscores the fact that ablation treats the arrhythmia symptom, but may not fully resolve the underlying pathology that drives thromboembolic risk. Therefore, the probability of stroke is overwhelmingly dependent on the CHA2DS2-VASc score, not on the ability to return to intense training. If OAC is required, the athlete must be counseled that contact or high-trauma sports are contraindicated due to bleeding risk.11
III. Suggested Course of Action: Detailed Training and Clinical Protocols
The course of action for the Masters athlete (50+) with treated Afib should focus on risk mitigation and structured exercise for cardiac resilience.
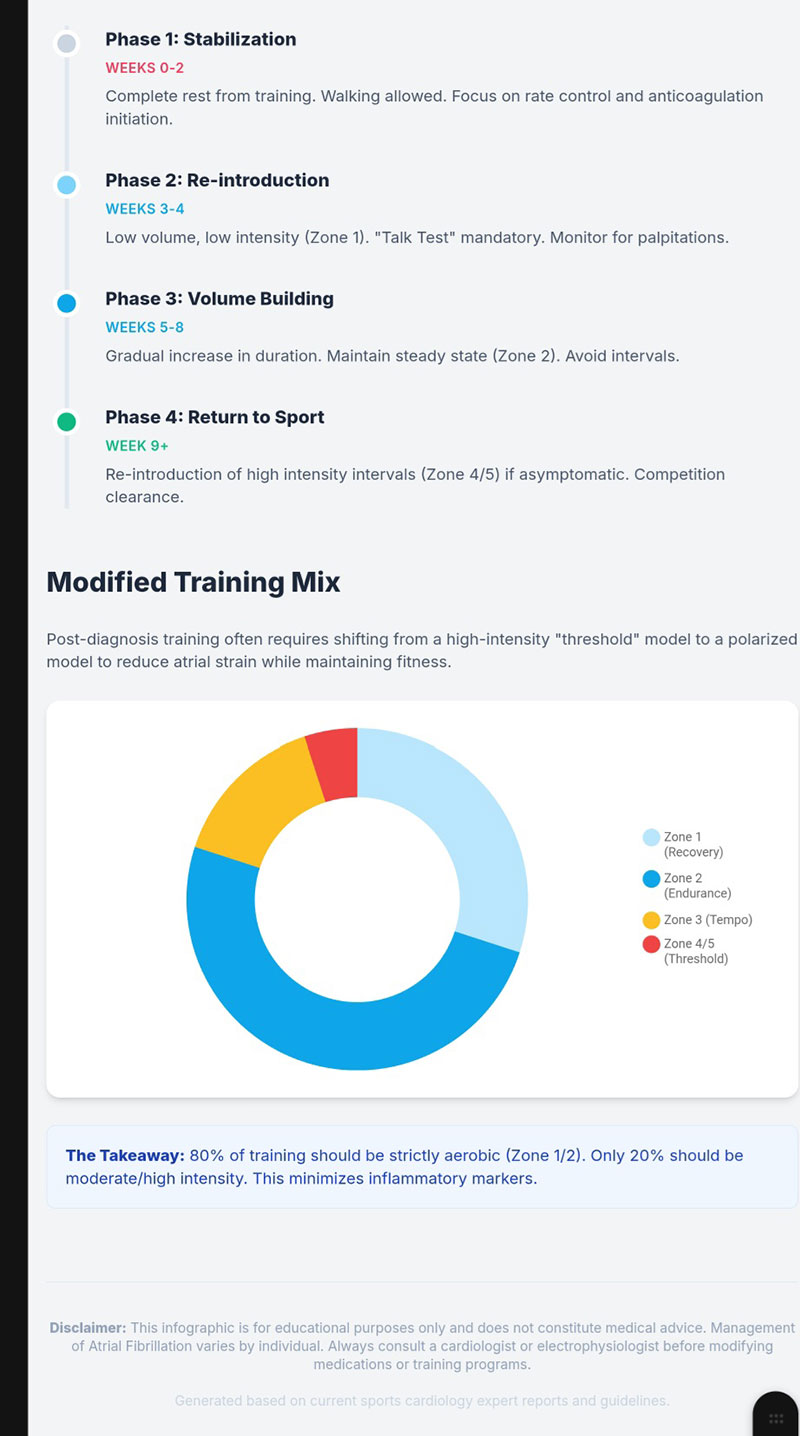
A. Phased Training Modification Protocol
The transition from a high-volume endurance regimen to a therapeutic regimen requires structured phasing and communication, especially regarding the established link between high-intensity training and Afib burden.5
| Phase | Duration | Activity/Goal | Clinical Rationale and Guidance |
| Phase 1: Immediate Post-Treatment Recovery | Initial 4–8 Weeks | Complete cessation or very light, non-competitive activity (e.g., walking). | Allows for myocardial healing and stabilization of sinus rhythm following ablation or cardioversion.12 Resumption of structured sports activity should begin only one month after ablation, provided the procedure is verified as successful.11 |
| Phase 2: Therapeutic Load & Maintenance | Ongoing (Long-Term) | Moderate-to-Vigorous Structured Aerobic Exercise, prioritizing shorter, higher-intensity intervals (AIT) over long, continuous duration. | The primary long-term objective is to maintain cardiorespiratory fitness (improved V02max) and cardiac function (improved Left Ventricular Ejection Fraction, LVEF 3), while avoiding the chronic volume strain that induced the Afib.13 The suggested target is approximately 210 minutes per week of moderate-to-vigorous aerobic exercise.4 |
The importance of using Aerobic Interval Training (AIT) in Phase 2 cannot be overstated, as subgroup analysis suggests interval training offers greater benefit in reducing AF recurrence compared to continuous training.3 A generalized return to long, slow distance training (>10 hours/week) should be actively discouraged, as this risks re-inducing the remodeling that caused the original arrhythmia.1
B. Clinical Management Considerations
- Antiarrhythmic Medication and Performance: Athletes are often intolerant of or unwilling to take medications like Beta-blockers, as these drugs profoundly reduce peak exercise capacity, measured by V02max.14 Catheter ablation is frequently preferred because it offers the possibility of eradicating Afib and allowing a return to competition without daily performance-limiting drug therapy.14 If “pill-in-the-pocket” Class I drugs (flecainide or propafenone) are used for acute cardioversion, the athlete must refrain from intensive sports until two half-lives of the drug have elapsed (up to 2 days) due to the risk of pro-arrhythmic effects during adrenergic stress.11
- Monitoring and Evaluation: All athletes must be managed in a specialized sports cardiology center.1 Exercise stress testing should be conducted using protocols that mimic the athlete’s sport to ensure the ventricular rate remains controlled during maximal exertion, confirming therapeutic efficacy.1
- Anticoagulation Status: OAC status must be re-evaluated continuously. In high-risk athletes (CHA2DS2-VASc >2), OAC must be continued indefinitely, even if Afib appears suppressed.4 This clinical requirement guides participation in sports; sports with high risk of bodily contact or trauma are strictly not recommended for anticoagulated individuals.11
IV. Summary and Integration of Lipid Management (Stoicescu et al., 2025)
The holistic management of a Masters athlete (50+) requires addressing not only the electrophysiological disorder (Afib) but also the generalized cardiovascular risk, including lipid metabolism. The provided review paper, “HDL Function Versus Small Dense LDL: Cardiovascular Benefits and Implications” 15, provides essential context for managing atherosclerotic risk (ASCVD) in this population.
A. Paper Summary: HDL Function Versus Small Dense LDL
The review by Stoicescu, Vacarescu, and Cozma highlights a significant paradigm shift in lipidology: the focus has moved away from High-Density Lipoprotein Cholesterol (HDL-C) concentration toward functional capacity and aggressive reduction of atherogenic particles.17
- HDL Focus: Function over Quantity: While HDL traditionally was considered cardioprotective, pharmacologically increasing HDL-C concentration—via agents like Niacin (AIM-HIGH, HPS2-THRIVE trials) or CETP inhibitors (ILLUMINATE, ACCELERATE trials)—did not consistently reduce cardiovascular events.16 The predictive and protective value lies instead in HDL functionality, particularly its Cholesterol Efflux Capacity (CEC), which represents its ability to remove cholesterol from macrophages in arterial plaques.16
- sdLDL: The Principal Atherogenic Target: Small Dense Low-Density Lipoprotein (sdLDL) particles are identified as critically atherogenic.16 Their physical characteristics—small size, higher density, and low antioxidant content—allow them to penetrate the arterial intima efficiently and undergo oxidative modification.15 Furthermore, their prolonged plasma half-life (up to 74 hours) increases their exposure time to the endothelial environment.15 Elevated sdLDL concentrations are strongly associated with increased ASCVD event risk (Adjusted HRs: 1.21 to 1.52).16
- Therapeutic Consensus: Current guidelines prioritize reducing the overall burden of atherogenic lipoproteins, measured pragmatically by non-HDL-C or Apolipoprotein B (ApoB), which effectively targets sdLDL and remnant particles. Statins and PCSK9 inhibitors remain the foundation of therapy, reducing LDL-C and ApoB.16
B. Third-Order Integration: Dual Risk Management Strategy
The physiological mechanisms driving Afib risk (remodeling/fibrosis) and those driving atherosclerotic risk (sdLDL accumulation/inflammation) often overlap in the aging athlete. The approach must be comprehensive.
The necessity of managing Afib recurrence through exercise moderation paradoxically supports optimizing lipid profile via lifestyle:
- Lifestyle Synergy: Structured physical activity (moderate-to-vigorous exercise) and appropriate dietary modifications (e.g., Mediterranean, rich in unsaturated fats like olive oil 16, and low in refined carbohydrates) simultaneously address both cardiac risks. These changes improve overall cardiometabolic profile, enhance HDL functional capacity (increasing CEC and antioxidant potential), and reduce plasma triglyceride levels, thereby diminishing the hepatic production of sdLDL.16
- Targeted Residual Risk Mitigation (Omega-3): Given the high ASCVD risk associated with sdLDL and remnant particles, pharmacological intervention may be warranted if hypertriglyceridemia (e.g., > 150 mg/dL) persists despite optimal statin therapy and lifestyle changes. High-dose pharmaceutical-grade Eicosapentaenoic Acid (EPA) demonstrated a 25% relative risk reduction in major cardiovascular events in the REDUCE-IT trial.16 This is a targeted therapy for the residual risk driven by sdLDL.
- Critical Nuance in EPA Use: A vital consideration for a patient with established Afib is the recognized possibility of increased Afib incidence associated with high-dose omega-3 fatty acids.16 The decision to use high-dose EPA requires careful consultation with the electrophysiologist to balance the certain benefit of ASCVD risk reduction against the potential for exacerbating the underlying arrhythmia.
V. Conclusions and Recommendations
For the Masters athlete (age 50+) successfully treated for Atrial Fibrillation, the clinical data strongly indicate that continued intense training represents an elevated, medically unacceptable risk to long-term cardiac stability. The need to slow and restructure intense training is a mandatory component of therapy, not a subjective lifestyle choice.
The statistical probabilities overwhelmingly support intervention:
- The probability of Afib recurrence and progression (e.g., to atypical flutter) remains high if the athlete maintains chronic, high-volume endurance training, as this perpetuates the underlying atrial fibrosis.8
- Implementing a structured, therapeutic exercise dose (approximately 210 minutes per week of moderate-to-vigorous activity, favoring intervals) actively reduces the probability of AF recurrence (RR 82).3
- The probability of a stroke event increases substantially (HR > 2.5) if a high-risk athlete (CHA2DS2-VASc >2) prematurely discontinues OAC, underscoring that rhythm stability does not negate thromboembolic risk.4
Recommended Course of Action
- Mandatory Training Shift: The athlete must transition their training goal from maximal endurance performance to cardiovascular health maintenance. This involves reducing volume below chronic high-dose thresholds (i.e., less than 10 hours per week of high-intensity activity) and emphasizing structured interval training for sustained fitness and reduced Afib burden.
- Stroke Prevention Adherence: OAC status must adhere strictly to guideline recommendations based on the CHA2DS2-VASc score. For most Masters athletes over 50 with treated Afib, continued OAC is required, necessitating the avoidance of contact or high-trauma sports.
- Holistic Risk Management: Integrate the management of Afib with the control of atherosclerotic risk (ASCVD). Prioritize lifestyle factors (dietary fat composition, carbohydrate restriction) that enhance HDL function and reduce the highly atherogenic sdLDL particles.16 Any adjunctive therapy, such as high-dose EPA for hypertriglyceridemia, requires careful consideration due to the potential interaction with Afib burden.
- Expert Monitoring: The athlete’s return to play and training intensity must be guided by a cardiology team specializing in sports electrophysiology, using serial monitoring and exercise stress testing to confirm rhythm and rate control during exertion.1
References
- Mont L, Elosua R, Brugada J. Endurance sport practice as a risk factor for atrial fibrillation and atrial flutter. Europace. 2009;11(1):11-17. doi:10.1093/europace/eun289
- Malmo V, Nes BM, Amundsen BH, et al. Aerobic Interval Training Reduces the Burden of Atrial Fibrillation in the Short Term: A Randomized Trial. Circulation. 2016;133(5):466-473. doi:10.1161/CIRCULATIONAHA.115.018220
- Fukata E, Hardani R, Mukti N, Pranawa F, Rusnanta F, Rizal A. Physical Exercise Intervention Improves Cardiac Function and Reduce Recurrences in Non-permanent Atrial Fibrillation: A Systematic Review and Meta-analysis. J Saudi Heart Assoc. 2025;37(4):1459. Published 2025 Oct 10. doi:10.37616/2212-5043.1459
- Noseworthy PA, Yao X, Deshmukh AJ, et al. Patterns of Anticoagulation Use and Cardioembolic Risk After Catheter Ablation for Atrial Fibrillation. J Am Heart Assoc. 2015;4(11):e002597. Published 2015 Nov 5. doi:10.1161/JAHA.115.002597
- Guasch E, Mont L. Diagnosis, pathophysiology, and management of exercise-induced arrhythmias. Nat Rev Cardiol. 2017;14(2):88-101. doi:10.1038/nrcardio.2016.173
- Pelliccia A, Maron BJ, Di Paolo FM, et al. Prevalence and clinical significance of left atrial remodeling in competitive athletes. J Am Coll Cardiol. 2005;46(4):690-696. doi:10.1016/j.jacc.2005.04.052
- Benito B, Gay-Jordi G, Serrano-Mollar A, et al. Cardiac arrhythmogenic remodeling in a rat model of long-term intensive exercise training. Circulation. 2011;123(1):13-22. doi:10.1161/CIRCULATIONAHA.110.938282
- Katritsis G, Calkins H. Catheter Ablation of Atrial Fibrillation – Techniques and Technology. Arrhythm Electrophysiol Rev. 2012;1(1):29-33. doi:10.15420/aer.2012.1.29
- Calvo N, Mont L, Tamborero D, et al. Efficacy of circumferential pulmonary vein ablation of atrial fibrillation in endurance athletes. Europace. 2010;12(1):30-36. doi:10.1093/europace/eup320
- Heidbüchel H, Panhuyzen-Goedkoop N, Corrado D, et al. Recommendations for participation in leisure-time physical activity and competitive sports in patients with arrhythmias and potentially arrhythmogenic conditions Part I: Supraventricular arrhythmias and pacemakers. Eur J Cardiovasc Prev Rehabil. 2006;13(4):475-484. doi:10.1097/01.hjr.0000216543.54066.72
- Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021;42(1):17-96. doi:10.1093/eurheartj/ehaa605
- Elliott AD, Mahajan R, Lau DH, Sanders P. Atrial Fibrillation in Endurance Athletes: From Mechanism to Management. Cardiol Clin. 2016;34(4):567-578. doi:10.1016/j.ccl.2016.06.006
- Menezes AR, Lavie CJ, De Schutter A, et al. Lifestyle modification in the prevention and treatment of atrial fibrillation. Prog Cardiovasc Dis. 2015;58(2):117-125. doi:10.1016/j.pcad.2015.07.001
- Lobo HM, Naves ÍG, Marçal SB, Canzi CC, Rodrigues ABS, Menezes AS Jr. Atrial Fibrillation in Endurance Training Athletes: Scoping Review. Rev Cardiovasc Med. 2023;24(6):155. Published 2023 May 26. doi:10.31083/j.rcm2406155
- Stoicescu C, Vacarescu C, Cozma D. HDL Function Versus Small Dense LDL: Cardiovascular Benefits and Implications. J Clin Med. 2025;14(14):4945. Published 2025 Jul 12. doi:10.3390/jcm14144945
- Bhatt DL, Steg PG, Miller M, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N Engl J Med. 2019;380(1):11-22. doi:10.1056/NEJMoa1812792
- Rohatgi A, Khera A, Berry JD, et al. HDL cholesterol efflux capacity and incident cardiovascular events. N Engl J Med. 2014;371(25):2383-2393. doi:10.1056/NEJMoa1409065