
1. Introduction: Challenging the Paradigm of Permanent Progression
The management of coronary artery disease (CAD) has traditionally been viewed through the lens of “risk management.” In this paradigm, pharmacological interventions such as statins and procedural approaches such as Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Grafting (CABG) are deployed to slow the expected progression of disease. However, these approaches primarily address late-stage manifestations—the “downstream” consequences—rather than the “upstream” cellular and molecular drivers of plaque formation and instability [1], [9].
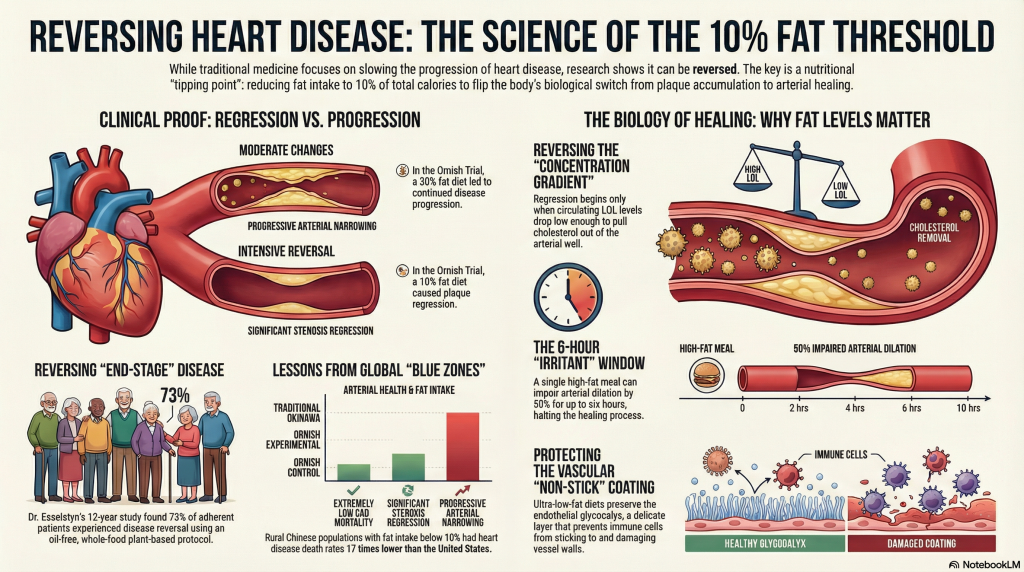
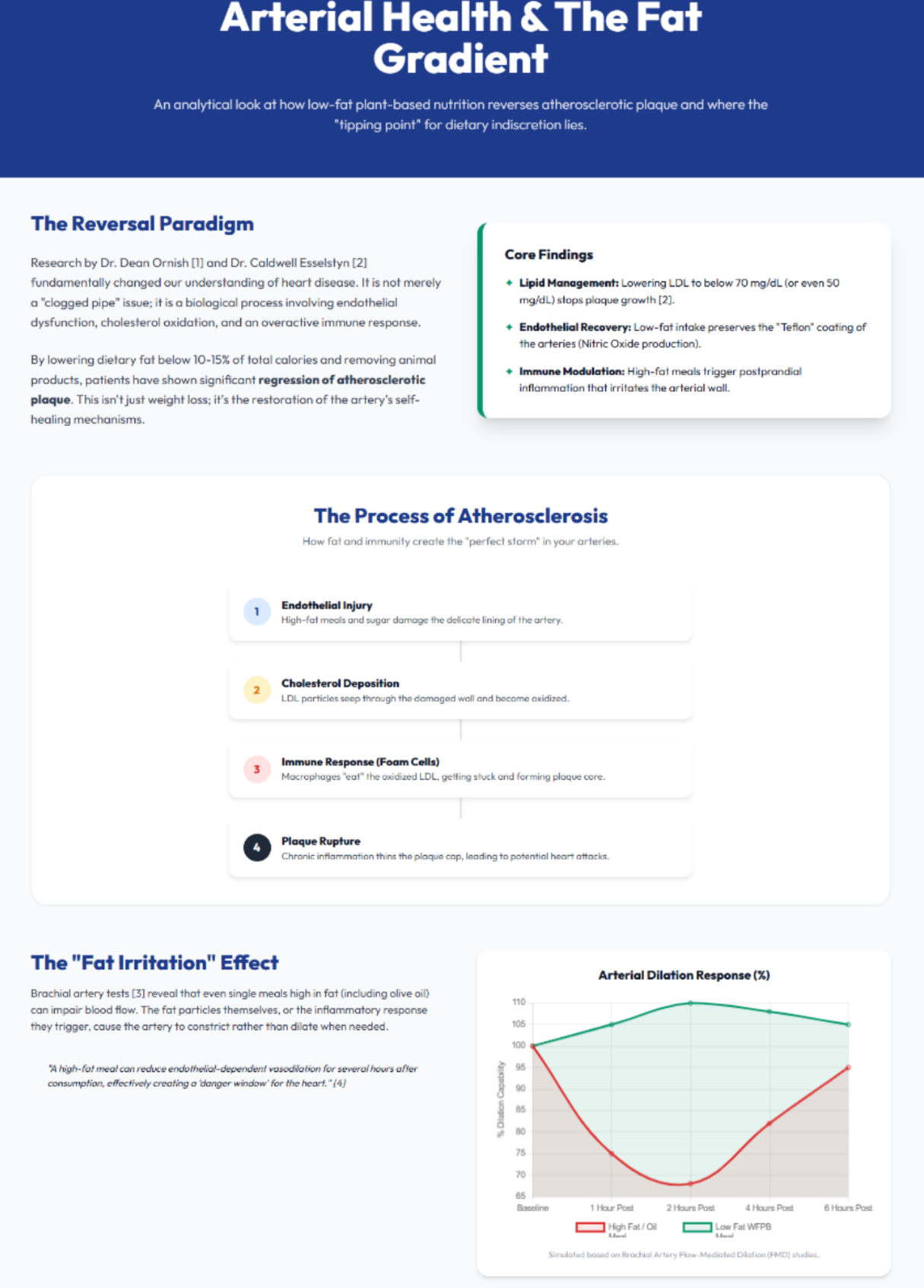
The emerging clinical consensus among lifestyle medicine researchers is that CAD is not an inevitable consequence of aging, but a reversible condition strongly modulated by nutritional choices. Central to this reversal is the implementation of an ultra-low-fat (approximately 10% of total calories), oil-free, whole-food plant-based (WFPB) diet [3], [7]. This report examines why the 10% threshold is biologically meaningful and how modern dietary “indiscretions” can halt—or reverse—the healing trajectory of the arterial wall.

2. The Quantitative Foundations of Coronary Reversal
The clinical validation of atherosclerotic regression was established most rigorously by the Lifestyle Heart Trial, a landmark prospective, randomized controlled study designed to test whether intensive lifestyle modification could affect the progression of coronary lesions without lipid-lowering medications [1].
2.1 The Ornish Lifestyle Heart Trial
The experimental group in this trial adhered to a nutritional protocol consisting of a 10% fat whole-foods vegetarian diet, supplemented by aerobic exercise, stress management training, and smoking cessation [1], [3]. Using quantitative coronary angiography (QCA), investigators demonstrated a clear divergence between the experimental and control groups.
In the first year, the experimental group showed an average diameter stenosis regression from 40.0% to 37.8%. In contrast, the control group—following a “moderate” 30% fat diet consistent with standard recommendations at the time—showed progression from 42.7% to 46.1% [1]. When extended to five years, the experimental group sustained regression to 37.3%, while the control group worsened to 51.9% [5]. This finding underscores that “moderate” changes do not yield moderate regression; in advanced disease, they often yield no regression at all [6].
2.2 The Esselstyn Longitudinal Study
Dr. Caldwell Esselstyn’s work at the Cleveland Clinic further refined the WFPB protocol by removing all oils and animal products entirely. His 12-year longitudinal study followed patients with advanced CAD who had been told they were “end-stage.” By maintaining total serum cholesterol below 150 mg/dL and LDL cholesterol below 80 mg/dL through nutrition alone, 73% of adherent patients experienced disease reversal as assessed by angiography and clinical outcomes [2].
| Study Cohort | Intervention Type | Baseline Stenosis (%) | Outcome |
| Ornish Experimental | 10% Fat WFPB + Lifestyle | 40.0 | Significant Regression [1] |
| Ornish Control | Standard Care (~30% Fat) | 42.7 | Progressive Stenosis [1] |
| Esselstyn Cohort | Oil-Free WFPB Diet | Severe | Cessation of Angina / Regression [2] |
| CORDIOPREV | Mediterranean vs Low-Fat (Secondary Prevention) | CHD baseline | Reduced events vs comparator diet [8] |
3. The Lipid–Immune Interface: Mechanisms of Plaque Stability
To understand why fat must be restricted so severely for regression, one must appreciate the “concentration gradient” across the arterial wall. Atherosclerotic plaque is initiated by the retention, accumulation, and modification of low-density lipoprotein (LDL) particles within the sub-endothelial space [9], [10].
3.1 The Concentration Gradient and Efflux
When circulating LDL levels are high, the gradient favors movement of LDL into the arterial wall. Once retained, LDL becomes modified through oxidation and related biochemical processes [9]. Modified LDL is recognized by the innate immune system as a danger signal. Monocytes are recruited and differentiate into macrophages, which ingest modified LDL and become lipid-laden “foam cells,” a hallmark of plaque development [10].
Regression becomes possible when circulating LDL falls low enough (often below ~70 mg/dL) that the gradient reverses, enabling net efflux of cholesterol out of the arterial wall through Reverse Cholesterol Transport [4]. In clinical practice, an ultra-low-fat dietary pattern is often necessary to achieve these LDL levels without high-dose statin dependence [2].
3.2 Metaflammation and TLR4
High-fat meals do more than elevate LDL; they can initiate “metaflammation.” Saturated fatty acids (SFAs) can activate Toll-like receptor 4 (TLR4), a pattern-recognition receptor best known for detecting microbial toxins [11]. TLR4 activation promotes NF-κB signaling and increases cytokine production such as IL-6 and TNF-α [11]. These inflammatory mediators can destabilize plaque by weakening the fibrous cap, increasing vulnerability to rupture and thrombosis [9].
4. The “Irritant” Effect: Endothelial Dysfunction
Patients commonly describe a feeling of “irritation” or “sluggishness” after high-fat meals. This is not merely subjective; it reflects acute endothelial dysfunction.
4.1 Nitric Oxide Bioavailability
The endothelium—the single-cell layer lining blood vessels—produces Nitric Oxide (NO), a key mediator of vasodilation and vascular “non-stick” signaling. NO reduces leukocyte adhesion and platelet activation, helping maintain an anti-atherogenic surface [13].
After a high-fat meal (including meals high in animal fat or refined plant oils), triglyceride-rich lipoproteins rise in circulation, producing postprandial lipemia and increased oxidative stress [14]. Reactive oxygen species neutralize NO, converting it into peroxynitrite and sharply reducing functional vasodilatory signaling [12], [13].
4.2 Flow-Mediated Dilation (FMD)
Flow-Mediated Dilation (FMD) studies show that within approximately 2 to 4 hours of a single high-fat meal, arterial dilation capacity can decline by roughly 50% [13]. This impairment can persist for up to 6 hours. With multiple high-fat meals per day, the vasculature can remain in a near-continuous state of impaired dilation and inflammatory tone [14].
5. The Biological Barrier: The Endothelial Glycocalyx
A critical but often overlooked component of vascular health is the endothelial glycocalyx—a delicate, gel-like surface layer that coats the luminal side of blood vessels. It functions as both a mechanotransducer and a physical barrier limiting LDL and immune cell interactions with endothelial membranes [15], [19].
When intact, the glycocalyx reduces leukocyte adhesion and helps prevent LDL infiltration. However, metabolic stressors such as hyperglycemia and inflammatory signals can cause the glycocalyx to shed into circulation [17]. Experimental evidence also demonstrates that exposure to oxidized LDL rapidly reduces glycocalyx thickness, leaving the vessel surface more adhesive and vulnerable to injury [16]. Dietary patterns that drive recurrent postprandial lipemia and oxidative stress can therefore contribute to glycocalyx dysfunction and impaired vascular recovery [18]. Restoration of glycocalyx integrity is a plausible mechanistic target of sustained ultra-low-fat, whole-food nutritional protocols [19].
6. Epidemiological Evidence: Lessons from Okinawa and Rural China
The historical diets of Okinawans and rural Chinese provide population-level evidence of the capacity to live with minimal coronary disease.
6.1 The Traditional Okinawan Diet
Before Westernization, Okinawans had among the highest life expectancy and lowest rates of cardiovascular disease globally [21]. Analyses of their traditional pre-1960 diet indicate macronutrient distribution of approximately 85% carbohydrate, 9% protein, and 6% fat [21]. The primary staple was the purple sweet potato, rich in fiber and antioxidant phytochemicals [21].
6.2 The China Study
In rural China during the 1970s and 1980s, investigators reported that in some counties the death rate from heart disease was extremely low [20]. Average fat intake was often below 10%, and mean serum cholesterol was approximately 127 mg/dL—levels considered “low” by Western standards, yet associated with markedly reduced rates of Western chronic disease patterns [20].
| Population | Fat Intake (%) | Primary Carb | CAD Mortality (vs US) |
| Rural China | <10 | Grains/Legumes | 1/17th [20] |
| Traditional Okinawa | 6 | Sweet Potato | Extremely Low [21] |
| Modern USA | 35+ | Refined Sugars | High [21] |
7. The “Crossover Limit”: The Danger of Nutritional Indiscretion
A common question is whether a “cheat meal”—such as fried chicken or a donut—is truly damaging. From the standpoint of regression biology, these indiscretions can temporarily halt arterial healing and reintroduce biochemical conditions that favor dysfunction.
- The 6-Hour Window: A single high-fat meal can induce approximately 6 hours of impaired endothelial responsiveness [12], [13].
- Glycocalyx Damage: Metabolic stressors—including hyperglycemia and oxidative stress—promote shedding of the protective glycocalyx [17], [18].
- Immune Re-Activation: For a patient in a “cooling” phase of plaque stabilization, a high-fat meal may re-activate TLR4 signaling and amplify inflammatory cascades that undermine cap stability [11].
For individuals with severe CAD, the “crossover limit” is low. Regression requires a stable biochemical environment. Frequent dietary “cheats” can prevent sustained low LDL and low inflammatory pressure, limiting the body’s ability to clear lipid burden from lesions and restore endothelial function [2], [4].
8. Strategic Conclusions and Clinical Synthesis
The evidence from clinical trials, epidemiological observation, and vascular biology supports the conclusion that the 10% fat threshold can be a critical determinant of atherosclerotic regression. Moderate-fat diets (25–30% fat) may support primary prevention and risk reduction, but often lack the biochemical intensity required for regression in established lesions [7], [8].
The vascular “irritation” described by patients reflects real postprandial physiology: oxidative stress, impaired nitric oxide bioavailability, and endothelial surface layer vulnerability. For the patient seeking regression, the clinical objective is a sustained environment of low LDL, reduced inflammatory signaling, and minimal postprandial lipid burden. This is achieved through a nutritional pattern that is not merely “mostly plants,” but strictly low in total fat and free of refined oils [2], [3]. By addressing root drivers—cholesterol retention and immune activation—rather than managing symptoms alone, an ultra-low-fat WFPB protocol provides a credible, non-surgical pathway toward comprehensive cardiovascular health.

References
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336(8708):129-133. doi:10.1016/0140-6736(90)91656-u
- Esselstyn CB Jr, Ellis SG, Medendorp SV, Crowe TD. A strategy to arrest and reverse coronary artery disease: a 5-year longitudinal study of a single physician’s practice. J Fam Pract. 1995;41(6):560-568.
- Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001-2007. doi:10.1001/jama.280.23.2001
- Roberts WC. It’s the cholesterol, stupid!. Am J Cardiol. 2010;106(9):1364-1366. doi:10.1016/j.amjcard.2010.09.022
- Gould KL, Ornish D, Scherwitz L, et al. Changes in myocardial perfusion abnormalities by positron emission tomography after long-term, intense risk factor modification. JAMA. 1995;274(11):894-901. doi:10.1001/jama.1995.03530110056036
- Varady KA, Lamarche B, Santosa S, Demonty I, Charest A, Jones PJ. Effect of weight loss resulting from a combined low-fat diet/exercise regimen on low-density lipoprotein particle size and distribution in obese women. Metabolism. 2006;55(10):1302-1307. doi:10.1016/j.metabol.2006.05.014
- Choi EY, Allen K, McDonnough M, Massera D, Ostfeld RJ. A plant-based diet and heart failure: case report and literature review. J Geriatr Cardiol. 2017;14(5):375-378. doi:10.11909/j.issn.1671-5411.2017.05.003
- Delgado-Lista J, Alcala-Diaz JF, Torres-Peña JD, et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. Lancet. 2022;399(10338):1876-1885. doi:10.1016/S0140-6736(22)00122-2
- Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524-533. doi:10.1038/s41586-021-03392-8
- Glass CK, Witztum JL. Atherosclerosis. the road ahead. Cell. 2001;104(4):503-516. doi:10.1016/s0092-8674(01)00238-0
- Rocha VZ, Libby P. Obesity, inflammation, and atherosclerosis. Nat Rev Cardiol. 2009;6(6):399-409. doi:10.1038/nrcardio.2009.55
- Rouyer O, Auger C, Charles AL, et al. Effects of a High Fat Meal Associated with Water, Juice, or Champagne Consumption on Endothelial Function and Markers of Oxidative Stress and Inflammation in Young, Healthy Subjects. J Clin Med. 2019;8(6):859. Published 2019 Jun 15. doi:10.3390/jcm8060859
- Lefèbvre PJ, Scheen AJ. The postprandial state and risk of cardiovascular disease. Diabet Med. 1998;15 Suppl 4:S63-S68. doi:10.1002/(sici)1096-9136(1998120)15:4+3.3.co;2-z
- Plotnick GD, Corretti MC, Vogel RA. Effect of antioxidant vitamins on the transient impairment of endothelium-dependent brachial artery vasoactivity following a single high-fat meal. JAMA. 1997;278(20):1682-1686.
- Milusev A, Rieben R, Sorvillo N. The Endothelial Glycocalyx: A Possible Therapeutic Target in Cardiovascular Disorders. Front Cardiovasc Med. 2022;9:897087. Published 2022 May 13. doi:10.3389/fcvm.2022.897087
- Vink H, Constantinescu AA, Spaan JA. Oxidized lipoproteins degrade the endothelial surface layer : implications for platelet-endothelial cell adhesion. Circulation. 2000;101(13):1500-1502. doi:10.1161/01.cir.101.13.1500
- Nieuwdorp M, van Haeften TW, Gouverneur MC, et al. Loss of endothelial glycocalyx during acute hyperglycemia coincides with endothelial dysfunction and coagulation activation in vivo. Diabetes. 2006;55(2):480-486. doi:10.2337/diabetes.55.02.06.db05-1103
- Calles-Escandon J, Cipolla M. Diabetes and endothelial dysfunction: a clinical perspective. Endocr Rev. 2001;22(1):36-52. doi:10.1210/edrv.22.1.0417
- Broekhuizen LN, Lemkes BA, Mooij HL, et al. Effect of sulodexide on endothelial glycocalyx and vascular permeability in patients with type 2 diabetes mellitus. Diabetologia. 2010;53(12):2646-2655. doi:10.1007/s00125-010-1910-x
- Gates JR, Parpia B, Campbell TC, Junshi C. Association of dietary factors and selected plasma variables with sex hormone-binding globulin in rural Chinese women. Am J Clin Nutr. 1996;63(1):22-31. doi:10.1093/ajcn/63.1.22
- Willcox BJ, Willcox DC, Todoriki H, et al. Caloric restriction, the traditional Okinawan diet, and healthy aging: the diet of the world’s longest-lived people and its potential impact on morbidity and life span. Ann N Y Acad Sci. 2007;1114:434-455. doi:10.1196/annals.1396.037