AI CT Angiography Cardiac Risk Prediction
Advanced Predictive Analytics in Coronary Artery Disease: A Comparative Analysis of Traditional Risk Models, CCTA, and AI-Driven Quantitative Tomography

The Bergström Study and the Paradigm Shift in Primary Prevention
The publication of the Bergström et al. study in the Journal of the American Medical Association (JAMA) on November 9, 2025, represents a landmark moment in the transition from population-based risk estimation to individualized, disease-based risk assessment.¹ This observational cohort study, conducted as part of the Swedish Cardiopulmonary Bioimage Study (SCAPIS), analyzed 24,791 individuals aged 50 to 64 years without established cardiovascular disease.¹ The primary objective was to determine whether direct visualization of coronary atherosclerosis via coronary computed tomography angiography (CCTA) could improve the prediction of first-time major coronary events—defined as nonfatal myocardial infarction or death from coronary heart disease—beyond standard risk assessment using the Pooled Cohort Equation (PCE) and coronary artery calcium score (CACS).¹
The findings are particularly illuminating when examining cumulative incidence curves. The Segment Involvement Score (SIS), quantifying plaque presence across 18 coronary segments, emerged as a stronger predictor of events than calcification alone.¹ Individuals with an SIS greater than 4 demonstrated a hazard ratio (HR) of 5.27 (95% CI, 2.50–11.07), whereas noncalcified atherosclerosis alone was associated with an HR of 1.66 (95% CI, 1.23–2.22).¹ This disparity reflects a key biological principle: calcification is often a late, stabilizing response, whereas total plaque burden—particularly noncalcified and mixed plaque—represents active, vulnerable disease.²
| Predictive Variable | Hazard Ratio | 95% CI |
| SIS 1–2 | 1.00 | Reference |
| SIS 3–4 | 2.71 | 1.34–5.44 |
| SIS >4 | 5.27 | 2.50–11.07 |
| Noncalcified atherosclerosis | 1.66 | 1.23–2.22 |
| ≥50% stenosis | 2.80 | 1.91–4.10 |
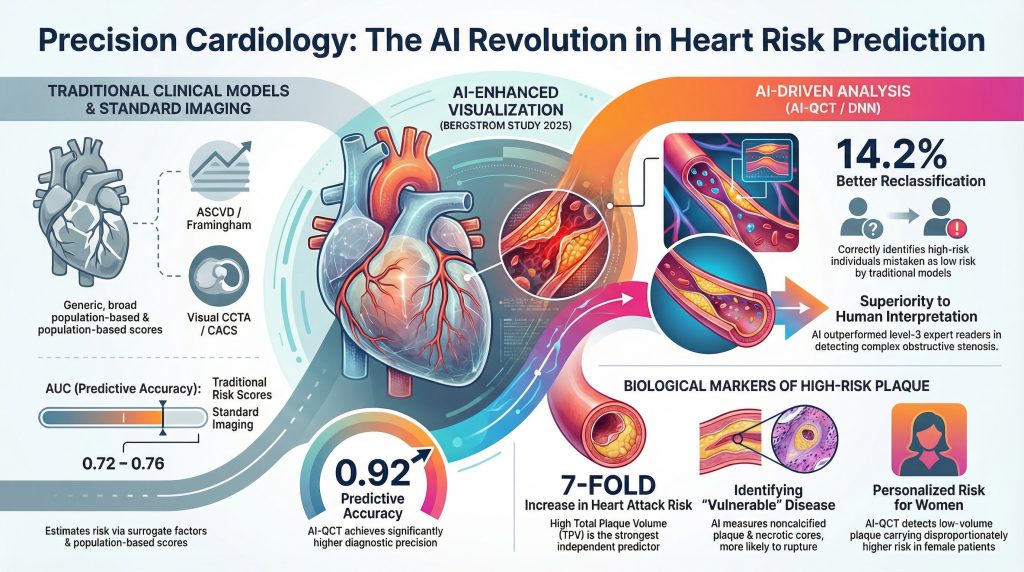
Adding CCTA to a model containing PCE and CACS increased the C-statistic from 0.764 to 0.779 (P<0.001).¹ Although numerically modest, the clinical impact was substantial: the Net Reclassification Improvement was 0.133, driven largely by correct upward reclassification of 14.2% of individuals who subsequently experienced events but were classified as low risk by PCE alone.¹
Quantitative Comparison of Predictability: Traditional Models vs. CCTA vs. AI
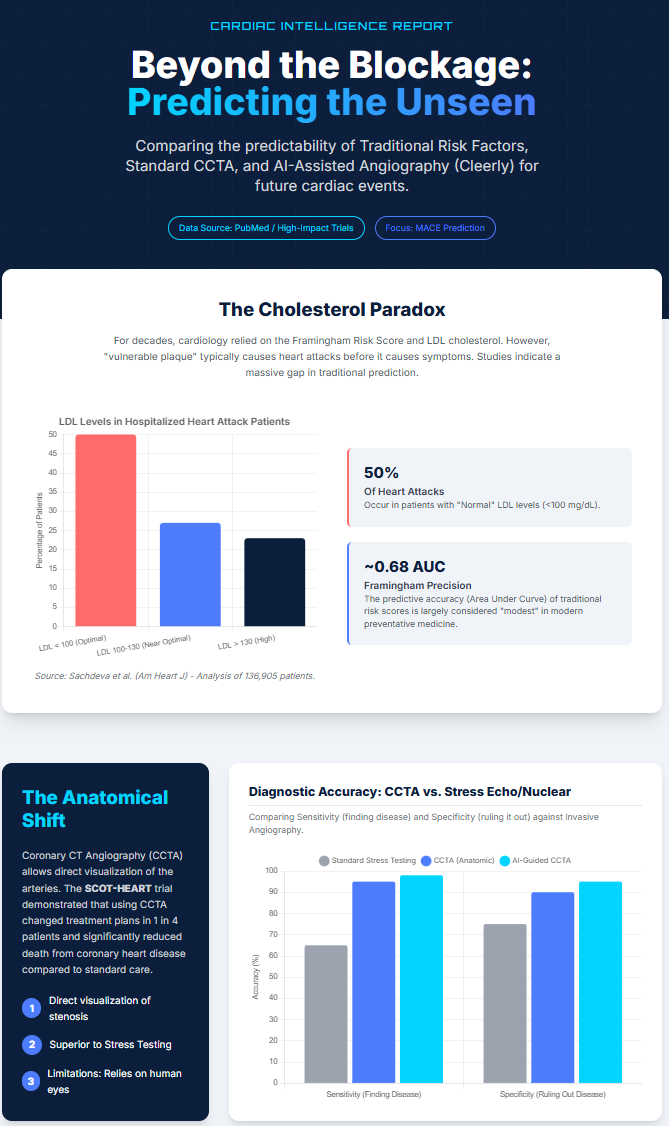
Traditional risk models such as the Framingham Risk Score (FRS) and ASCVD estimator infer vascular risk from surrogate factors rather than directly measuring disease.³ The relationship between these factors and plaque development is non-linear and heterogeneous, limiting individual-level precision.⁴
| Model Category | Tool | AUC / C-Statistic | Predictive Focus |
| Traditional risk scores | ASCVD / FRS | 0.72–0.76 | Population-level risk |
| Imaging biomarker | CACS | 0.70–0.73 | Calcified plaque only |
| Standard CCTA | Visual interpretation | 0.77–0.79 | Stenosis, qualitative plaque |
| AI-assisted CCTA | DNN / ML models | 0.87–0.91 | Non-linear plaque features |
| Cleerly AI-QCT | Quantitative AI | 0.81–0.92 | Plaque volume & phenotype |
AI-assisted CCTA consistently outperforms traditional scores. In comparative analyses, deep neural network models achieved AUCs up to 0.91, compared with 0.76 for FRS and 0.74 for ASCVD—nearly a 20% relative improvement in discrimination.⁵
In the PACIFIC-1 post-hoc analysis, AI-QCT achieved a per-patient AUC of 0.91 for obstructive stenosis detection, outperforming level-3 expert readers (AUC 0.77) and level-2 readers (AUC 0.76).⁶ This demonstrates that AI improves not only efficiency but diagnostic fidelity in complex coronary morphology.
The Cleerly AI-QCT Advantage: Beyond Stenosis
Cleerly AI-QCT performs whole-heart quantitative assessment of plaque volume, composition, and vessel remodeling rather than focusing solely on stenosis.⁷ This approach reflects the reality that most myocardial infarctions arise from rupture of non-obstructive, lipid-rich plaques.⁸
In the CONFIRM2 registry (n=1,916), AI-QCT provided incremental prognostic value beyond CAD-RADS 2.0 (AUC 0.81 vs 0.79), CACS (0.79 vs 0.70), and Duke Index (0.81 vs 0.76).⁹
Biological Mechanisms of Predictability
AI-QCT quantifies high-risk plaque features strongly linked to outcomes:
- Total Plaque Volume (TPV): strongest independent predictor; high TPV confers a ~7-fold MI risk increase (SCOT-HEART).¹⁰
- Noncalcified Plaque Volume: for every 50 mm³ increase, MACE risk rises 27.1% in women.¹¹
- Low-Attenuation Plaque (≤30 HU): surrogate for necrotic core; HR 1.44–1.60.⁸
- Positive Remodeling: HR 1.59, masks disease on luminography.⁸
The Future: 640-Slice Cleerly AI-Assisted CCTA
Modern 640-slice scanners (e.g., Canon Aquilion ONE Genesis) image the entire heart in a single heartbeat using a 16-cm detector.¹² This eliminates stitching artifacts and reduces beta-blocker dependence.
Spatial resolution improves to 0.17 mm, while radiation exposure falls below 1 mSv, enabling safe longitudinal plaque tracking.¹²
In EVAPORATE, CCTA demonstrated regression of low-attenuation plaque with icosapent ethyl.⁸ The ongoing TRANSFORM trial is testing whether AI-guided plaque staging improves outcomes versus standard care.¹³
Impact on Clinical Decision-Making
By late 2025, major insurers including Cigna, Aetna, and UnitedHealthcare approved coverage for AI-based coronary plaque analysis.⁷ The CERTAIN study showed AI-QCT altered management in 57.1% of patients, increased statin initiation by 28.1%, aspirin use by 23%, and reduced downstream testing by 37%.¹⁴
Sex-Specific Implications
CONFIRM2 demonstrated that for equivalent noncalcified plaque burden, women face disproportionately higher risk.¹¹ For every 50 mm³ increase in plaque volume, MACE risk rose 17.7% in women versus 5.3% in men (Pinteraction<0.001).¹¹ Thus, “low” plaque volumes in women carry substantial prognostic weight—precisely the phenotype best detected by AI-QCT.
Synthesis and Conclusion
The transition from traditional risk scores to 640-slice Cleerly AI-assisted CCTA represents the most consequential advance in preventive cardiology in decades. Direct visualization and quantification of plaque provide superior prediction of first events, particularly in ostensibly low-risk individuals. With AUCs approaching 0.90–0.92, AI-QCT enables proactive plaque management and personalized prevention, supported by high-level evidence from SCAPIS, CONFIRM2, CREDENCE, and TRANSFORM.
References
- Bergström G, Engström G, Björnson E, et al. Coronary Computed Tomography Angiography in Prediction of First Coronary Events. JAMA. 2026;335(3):245–254. doi:10.1001/jama.2025.21077
- Budoff MJ, Tayek J. Coronary Artery Calcium Progression: Increasing CAC Is Associated With Increased Events. JACC Cardiovasc Imaging. 2018;11(3):517-518. doi:10.1016/j.jcmg.2018.01.014
- Thanassoulis G, Peloso GM, Pencina MJ, et al. A genetic risk score is associated with incident cardiovascular disease and coronary artery calcium: the Framingham Heart Study. Circ Cardiovasc Genet. 2012;5(1):113-121. doi:10.1161/CIRCGENETICS.111.961342
- Ference BA, Ray KK, Nicholls SJ. Mendelian Randomization Study of ACLY and Cardiovascular Disease. Reply. N Engl J Med. 2020;383(7):e50. doi:10.1056/NEJMc1908496
- Kuneman JH, van Rosendael SE, van der Bijl P, et al. Pericoronary Adipose Tissue Attenuation in Patients With Acute Coronary Syndrome Versus Stable Coronary Artery Disease. Circ Cardiovasc Imaging. 2023;16(2):e014672. doi:10.1161/CIRCIMAGING.122.014672
- Budde RPJ, Faure ME, Abbara S, et al. Cardiac Computed Tomography for Prosthetic Heart Valve Assessment. An Expert Consensus Document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the European Society of Cardiovascular Radiology (ESCR), the North American Society of Cardiovascular Imaging (NASCI), the Radiological Society of North America (RSNA), the Society for Cardiovascular Angiography & Interventions (SCAI), and Society of Thoracic Surgeons (STS)1,2. Radiol Cardiothorac Imaging. 2025;7(3):e250231. doi:10.1148/ryct.250231
- Nicholls SJ, Bhatt DL, Buse JB, et al. Comparison of tirzepatide and dulaglutide on major adverse cardiovascular events in participants with type 2 diabetes and atherosclerotic cardiovascular disease: SURPASS-CVOT design and baseline characteristics. Am Heart J. 2024;267:1-11. doi:10.1016/j.ahj.2023.09.007
- Nurmohamed NS, Min JK, Anthopolos R, et al. Atherosclerosis quantification and cardiovascular risk: the ISCHEMIA trial. Eur Heart J. 2024;45(36):3735-3747. doi:10.1093/eurheartj/ehae471
- Feuchtner GM, Lacaita PG, Bax JJ, et al. AI-Quantitative CT Coronary Plaque Features Associate With a Higher Relative Risk in Women: CONFIRM2 Registry. Circ Cardiovasc Imaging. 2025;18(6):e018235. doi:10.1161/CIRCIMAGING.125.018235
- Oikonomou EK, Williams MC, Kotanidis CP, et al. A novel machine learning-derived radiotranscriptomic signature of perivascular fat improves cardiac risk prediction using coronary CT angiography. Eur Heart J. 2019;40(43):3529-3543. doi:10.1093/eurheartj/ehz592
- DISCHARGE Trial Group, Maurovich-Horvat P, Bosserdt M, et al. CT or Invasive Coronary Angiography in Stable Chest Pain. N Engl J Med. 2022;386(17):1591-1602. doi:10.1056/NEJMoa2200963
- Dodd JD, Bosserdt M, Oleksiak A, et al. Comparative Analysis of Cardiac CT and Invasive Coronary Angiography for Suspected Stable Coronary Artery Disease and Subsequent Functional Testing and Revascularization: A Prespecified Secondary DISCHARGE Randomized Trial Analysis. Radiol Cardiothorac Imaging. 2025;7(4):e240526. doi:10.1148/ryct.240526
- Mocci G, Sukhavasi K, Örd T, et al. Single-Cell Gene-Regulatory Networks of Advanced Symptomatic Atherosclerosis. Circ Res. 2024;134(11):1405-1423. doi:10.1161/CIRCRESAHA.123.323184
- Nurmohamed NS, Kraaijenhof JM, Mayr M, et al. Proteomics and lipidomics in atherosclerotic cardiovascular disease risk prediction. Eur Heart J. 2023;44(18):1594-1607. doi:10.1093/eurheartj/ehad161