
What do people on social media mean by “ketosis,” and does it automatically mean “healthier”?
Ketosis simply means your blood ketones (often β-hydroxybutyrate, βHB) are elevated because carbohydrate availability is low (fasting, very-low-carb diets) or because you ingested ketones.
That metabolic state can have specific, real physiologic effects—but “being in ketosis” is not the same thing as “reducing atherosclerosis risk,” “reversing heart disease,” or “living longer.” Whether ketosis helps or harms depends heavily on what foods create it and what it does to apoB/LDL, blood pressure, inflammation, body weight, and diet quality.
Do exogenous ketones (ketone drinks/esters) improve athletic performance?
 The evidence is mixed and context-dependent. The best-known ketone ester work shows that exogenous ketosis can change fuel use (more fat oxidation, less glycolysis) and has sometimes been associated with endurance performance effects in controlled settings, but results vary by dose, sport, intensity, co-ingested carbs, and GI tolerance (1–3).
The evidence is mixed and context-dependent. The best-known ketone ester work shows that exogenous ketosis can change fuel use (more fat oxidation, less glycolysis) and has sometimes been associated with endurance performance effects in controlled settings, but results vary by dose, sport, intensity, co-ingested carbs, and GI tolerance (1–3).
A major scientific point: ketone esters can raise βHB quickly and predictably, which is useful for studying ketosis without changing the whole diet. That’s a research advantage, not a guarantee of performance gains in the real world (4).
Conclusions: some athletes may see benefits in specific endurance contexts, but exogenous ketones are not a universally proven ergogenic aid; and GI side effects and practical cost/taste issues are real constraints (5).
Isn’t keto “proven” because it improves insulin sensitivity and weight loss quickly?
Short-term improvements in glucose control and weight are real for many people, especially in type 2 diabetes—often because carbohydrate restriction reduces glycemic load and can facilitate weight loss and medication reduction (6).
But two key scientific caveats:
- Durability is less impressive than the hype suggests. A major systematic review/meta-analysis found low/very-low-carb diets can increase diabetes remission at ~6 months, but the advantage tends to diminish by 12 months as adherence drops and differences narrow (6).
- Cardiovascular risk markers can move in different directions. In longer-term “nutritional ketosis” interventions for type 2 diabetes, many risk factors improve (weight, triglycerides, glycemia), but LDL-C can rise in some participants—an issue that matters because atherosclerosis is driven strongly by apoB/LDL particle burden (7,8).
Keto can be a useful therapeutic tool for glycemia and weight in some people, but it is not automatically the best choice for heart disease reversal or longevity, and lipid responses can be a deal-breaker for some.
What’s the strongest “hard evidence” that a low-fat whole-food plant-based pattern can reverse atherosclerosis?
 There are two landmark clinical lines of evidence often cited because they used objective coronary imaging and tracked clinical outcomes:
There are two landmark clinical lines of evidence often cited because they used objective coronary imaging and tracked clinical outcomes:
1) Ornish/Lifestyle Heart Trial (randomized):
Participants assigned to intensive lifestyle change including a very-low-fat, whole-foods vegetarian diet showed regression of coronary atherosclerosis vs. controls in the first year, and sustained benefits were reported in longer follow-up (9).
Five-year follow-up showed continued regression in the intensive group and more cardiac events in controls (10).
2) Esselstyn cohort (longitudinal clinical series):
A very-low-fat plant-based diet in patients with established CAD was associated with arrest and, in some cases, reversal of disease over years, with outcomes strongly linked to adherence (11).
Are these perfect studies? No—sample sizes were modest and lifestyle bundles include more than diet. But the direction and plausibility are powerful: when you dramatically reduce atherogenic lipoproteins and emphasize high-fiber, minimally processed plant foods, coronary disease progression can slow, stop, and sometimes regress.
If your goal is reversing atherosclerosis, the most direct clinical evidence base favors very-low-fat, whole-food plant-forward patterns paired with comprehensive risk-factor management (9–11). So clearly plant based diets win clearly in my opinion.
What about insulin sensitivity and weight loss on whole-food plant-based diets—is there evidence beyond “it sounds healthy”?
Yes—there are randomized trials showing meaningful metabolic benefits:
- In overweight adults, a low-fat plant-based intervention improved weight and insulin sensitivity and reduced metabolic risk factors (12).
- In type 2 diabetes, a randomized trial found a low-fat vegan diet improved glycemic control and cardiovascular risk factors compared with a conventional diabetes diet (13).
- A 2-year randomized weight-loss trial found a low-fat vegan diet produced sustained weight loss advantages compared with a more moderate low-fat diet in a real-world format (14).
Mechanistically, one consistent theme is that high-fiber, low–energy-density plant foods can promote spontaneous calorie reduction, and lowering intramyocellular/liver fat may improve insulin resistance—often without needing ketosis.
Conclusions: you don’t need ketosis to improve insulin sensitivity; well-designed plant-based diets can do it, and the approach often aligns better with heart-protective lipid targets (12–14).
If keto improves triglycerides and HDL, why isn’t it automatically heart-protective?
Because atherosclerosis risk is driven heavily by apoB-containing particles (LDL, VLDL remnants) and cumulative exposure over time.
In nutritional ketosis interventions, it’s common to see lower triglycerides and sometimes higher HDL, but some studies report higher LDL-C (and variable LDL particle effects) (7,8).
If LDL/apoB rises substantially—especially if the diet is high in saturated fat—this can conflict with the core lipid-lowering strategy used to prevent and treat atherosclerotic disease.
Metabolic “wins” don’t automatically cancel out a large rise in LDL/apoB.
What does the longevity evidence say—do the longest-lived populations look “keto”?
In human population studies, dietary patterns associated with lower mortality and lower ischemic heart disease risk generally skew plant-forward rather than very-low-carb/high-fat.
Two large prospective datasets often discussed in this context:
- Adventist Health Study-2: vegetarian dietary patterns were associated with lower all-cause mortality compared with nonvegetarian patterns (15).
- EPIC-Oxford (18+ years): vegetarians had a lower risk of ischemic heart disease than meat eaters (with nuanced findings for stroke that highlight the importance of nutrient adequacy—e.g., B12) (16).
These aren’t “whole-food plant-based” trials, and observational data can’t prove causation. But they’re consistent with a broad scientific pattern: diets centered on minimally processed plant foods are compatible with long-term cardiometabolic health and lower mortality.
The best longevity-linked dietary patterns in large cohorts look much closer to plant-forward than to strict keto.
So what’s the most evidence-based way to frame this for the general public?
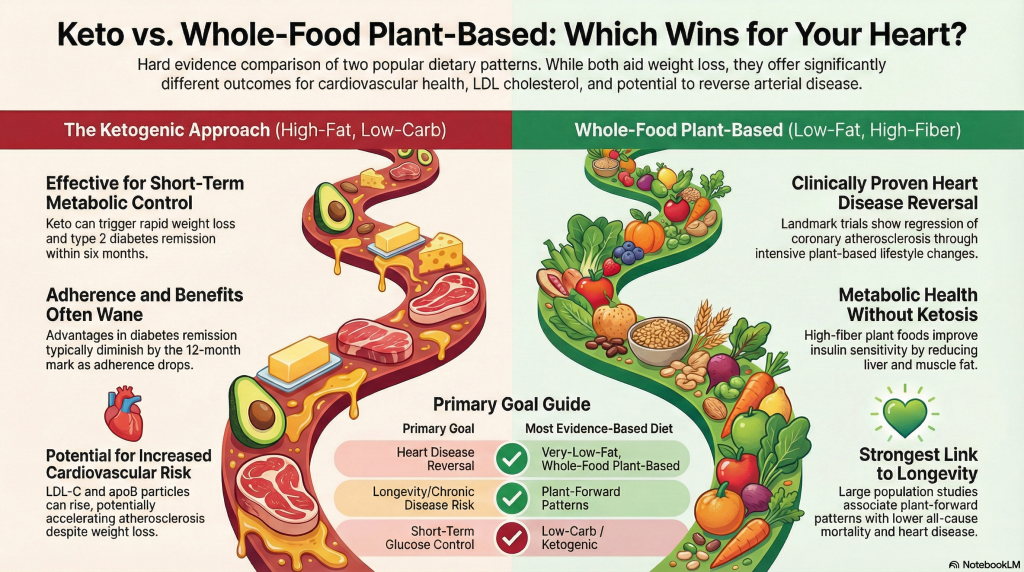
If your primary goal is heart disease reversal / atherosclerosis regression:
A very-low-fat, whole-food, plant-based pattern has some of the strongest direct clinical signals (including angiographic evidence) and aligns with LDL/apoB lowering (9–11).
If your primary goal is short-term glucose control or appetite/weight help:
Low-carb/keto can work for some—especially in type 2 diabetes—but the advantage may lessen over time and lipid responses should be monitored closely (6–8).
If your goal is longevity / chronic disease risk reduction at scale:
The strongest population evidence tilts toward plant-forward patterns (with attention to nutrient adequacy like B12) (15,16).
References
- Clarke K, Tchabanenko K, Pawlosky R, et al. Kinetics, safety and tolerability of (R)-3-hydroxybutyl (R)-3-hydroxybutyrate in healthy adult subjects. Regul Toxicol Pharmacol. 2012;63(3):401-408. doi:10.1016/j.yrtph.2012.04.008
- Cox PJ, Kirk T, Ashmore T, et al. Nutritional Ketosis Alters Fuel Preference and Thereby Endurance Performance in Athletes. Cell Metab. 2016;24(2):256-268. doi:10.1016/j.cmet.2016.07.010
- Evans M, McClure TS, Koutnik AP, Egan B. Exogenous Ketone Supplements in Athletic Contexts: Past, Present, and Future. Sports Med. 2022;52(Suppl 1):25-67. doi:10.1007/s40279-022-01756-2
- Soto-Mota A, Norwitz NG, Clarke K. Why a d-β-hydroxybutyrate monoester?. Biochem Soc Trans. 2020;48(1):51-59. doi:10.1042/BST20190240
- Stubbs BJ, Cox PJ, Kirk T, Evans RD, Clarke K. Gastrointestinal Effects of Exogenous Ketone Drinks are Infrequent, Mild, and Vary According to Ketone Compound and Dose. Int J Sport Nutr Exerc Metab. 2019;29(6):596-603. doi:10.1123/ijsnem.2019-0014
- Goldenberg JZ, Day A, Brinkworth GD, et al. Efficacy and safety of low and very low carbohydrate diets for type 2 diabetes remission: systematic review and meta-analysis of published and unpublished randomized trial data. BMJ. 2021;372:m4743. Published 2021 Jan 13. doi:10.1136/bmj.m4743
- Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-randomized Clinical Trial. Front Endocrinol (Lausanne). 2019;10:348. Published 2019 Jun 5. doi:10.3389/fendo.2019.00348
- Athinarayanan SJ, Hallberg SJ, McKenzie AL, et al. Impact of a 2-year trial of nutritional ketosis on indices of cardiovascular disease risk in patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19(1):208. Published 2020 Dec 8. doi:10.1186/s12933-020-01178-2
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336(8708):129-133. doi:10.1016/0140-6736(90)91656-u
- Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001-2007. doi:10.1001/jama.280.23.2001
- Esselstyn CB Jr, Ellis SG, Medendorp SV, Crowe TD. A strategy to arrest and reverse coronary artery disease: a 5-year longitudinal study of a single physician’s practice. J Fam Pract. 1995;41(6):560-568.
- Barnard ND, Scialli AR, Turner-McGrievy G, Lanou AJ, Glass J. The effects of a low-fat, plant-based dietary intervention on body weight, metabolism, and insulin sensitivity. Am J Med. 2005;118(9):991-997. doi:10.1016/j.amjmed.2005.03.039
- Barnard ND, Cohen J, Jenkins DJ, et al. A low-fat vegan diet improves glycemic control and cardiovascular risk factors in a randomized clinical trial in individuals with type 2 diabetes. Diabetes Care. 2006;29(8):1777-1783. doi:10.2337/dc06-0606
- Turner-McGrievy GM, Barnard ND, Scialli AR. A two-year randomized weight loss trial comparing a vegan diet to a more moderate low-fat diet. Obesity (Silver Spring). 2007;15(9):2276-2281. doi:10.1038/oby.2007.270
- Orlich MJ, Singh PN, Sabaté J, et al. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA Intern Med. 2013;173(13):1230-1238. doi:10.1001/jamainternmed.2013.6473
- Tong TYN, Appleby PN, Bradbury KE, et al. Risks of ischaemic heart disease and stroke in meat eaters, fish eaters, and vegetarians over 18 years of follow-up: results from the prospective EPIC-Oxford study. BMJ. 2019;366:l4897. Published 2019 Sep 4. doi:10.1136/bmj.l4897