
In a world of “biohacking” and rapid weight-loss trends, two dietary paradigms often clash: the Low-Fat Whole Food Plant-Based (WFPB) diet and the high-protein/high-fat Paleo/Ketogenic diets. While both claim to improve health, the scientific literature—specifically long-term clinical trials and centenarian studies—reveals a clear distinction between short-term metabolic shifts and long-term disease reversal.
This summary addresses the critical questions using hard evidence and peer-reviewed citations.
Can a Low-Fat Whole Food Plant-Based (WFPB) diet actually reverse heart disease?
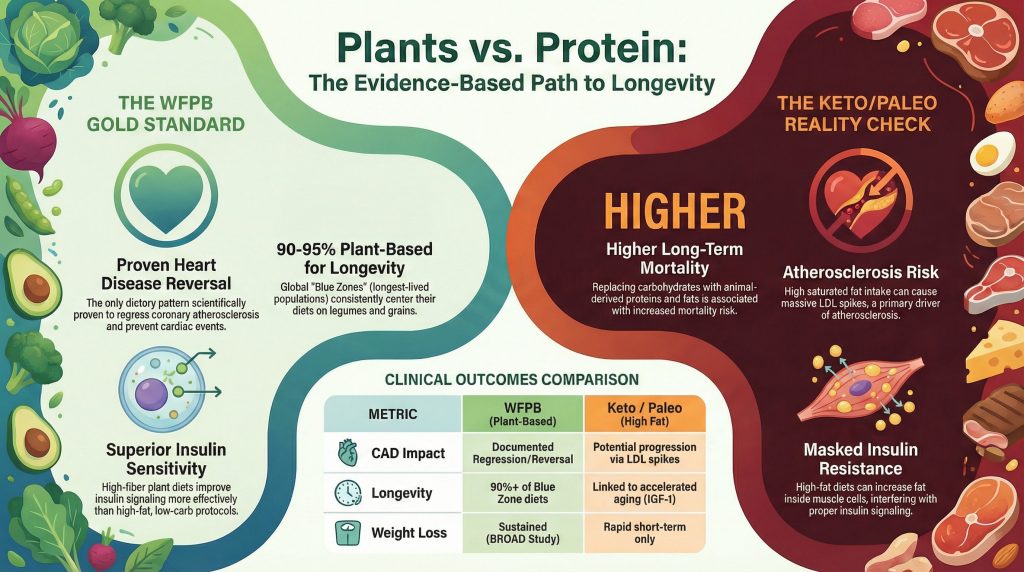
Yes. The WFPB diet is the only dietary pattern scientifically proven to not just prevent, but actually reverse coronary artery disease (CAD).
- The Evidence: Dr. Dean Ornish demonstrated in the Lifestyle Heart Trial that patients following a low-fat (10% fat) vegetarian diet, along with lifestyle changes, showed regression of coronary atherosclerosis after one year, with further improvement after five years. In contrast, the control group following “moderate” dietary changes saw their disease progress (Ornish et al., 1998).
- The Mechanism: A WFPB diet improves endothelial function—the ability of blood vessels to dilate—and lowers LDL cholesterol to “heart-attack proof” levels (typically <70 mg/dL). Dr. Caldwell Esselstyn’s 12-year study showed that 99.4% of patients who adhered to a WFPB diet avoided further major cardiac events (Esselstyn et al., 2014).
How does the “rapid weight loss” of Keto/Paleo compare to the long-term insulin sensitivity of WFPB?
While Ketogenic and Paleo diets are praised for rapid weight loss and immediate drops in blood glucose, these are often “short-term effects” that may mask underlying issues.
- Insulin Sensitivity: High-fat diets can actually increase intramyocellular lipids (fat inside muscle cells), which interferes with insulin signaling. While blood sugar may stay low because the patient is avoiding carbohydrates, the underlying insulin resistance often remains or worsens.
- The WFPB Advantage: Research shows that a high-carbohydrate, high-fiber WFPB diet improves insulin sensitivity more effectively over time. The Adventist Health Studies found that vegans had a 62% lower risk of developing type 2 diabetes compared to non-vegetarians, even after adjusting for body weight (Tonstad et al., 2009).
- Weight Loss: In the BROAD study, a 6-month randomized controlled trial, the WFPB group achieved greater weight loss at six and twelve months than any other trial that did not mandate regular exercise or calorie restriction (Wright et al., 2017).
What do the world’s longest-lived populations (The Blue Zones) tell us?
If longevity is the goal, we must look at the “Blue Zones”—regions where people live significantly longer than the global average (Okinawa, Sardinia, Loma Linda, Nicoya, and Ikaria).
- The Common Thread: None of the longest-lived populations follow a Ketogenic or high-protein Paleo diet. Their diets are consistently 90-95% plant-based, centered on legumes (beans, peas, lentils), whole grains, and tubers.
- Okinawa: Historically, the Okinawan diet was 69% sweet potatoes and very low in animal products (Willcox et al., 2007).
- Animal Protein and Aging: High animal protein intake is associated with increased levels of IGF-1 (Insulin-like Growth Factor 1), a hormone that promotes cell growth but is linked to accelerated aging and cancer (Levine et al., 2014).
Are there risks associated with long-term Keto/Paleo diets regarding longevity?
While Keto/Paleo diets can be effective for short-term insulin regulation in some, long-term epidemiological data suggest risks.
- Mortality Risk: A large-scale meta-analysis published in The Lancet Public Health found that both low-carbohydrate diets (<40% energy) and high-carbohydrate diets (>70% energy) were associated with increased mortality. However, risk was highest when carbohydrates were replaced by animal-derived protein and fat, whereas mortality decreased when carbohydrates were replaced by plant-based proteins and fats (Seidelmann et al., 2018).
- Atherosclerosis Risk: High-saturated fat intake, typical of many Keto/Paleo diets, significantly raises LDL cholesterol. The “Lean Mass Hyper-Responder” phenotype seen in some Keto practitioners involves massive LDL spikes, which is a primary driver of atherosclerosis (Nylander et al., 2023).
Conclusion: The Evidence-Based Choice
If the objective is the reversal of atherosclerosis and the maximization of lifespan, the evidence heavily favors a low-fat, whole food plant-based diet. While Paleo and Keto may provide temporary metabolic improvements via weight loss and carbohydrate restriction, they lack the proven track record for reversing our #1 killer—heart disease—and contradict the dietary patterns found in every long-lived population on Earth.
References
- Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD?. J Fam Pract. 2014;63(7):356-364b.
- Levine ME, Suarez JA, Brandhorst S, et al. Low protein intake is associated with a major reduction in IGF-1, cancer, and overall mortality in the 65 and younger but not older population. Cell Metab. 2014;19(3):407-417. doi:10.1016/j.cmet.2014.02.006
- Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001-2007. doi:10.1001/jama.280.23.2001
- Seidelmann SB, Claggett B, Cheng S, et al. Dietary carbohydrate intake and mortality: a prospective cohort study and meta-analysis. Lancet Public Health. 2018;3(9):e419-e428. doi:10.1016/S2468-2667(18)30135-X
- Tonstad S, Butler T, Yan R, Fraser GE. Type of vegetarian diet, body weight, and prevalence of type 2 diabetes. Diabetes Care. 2009;32(5):791-796. doi:10.2337/dc08-1886
- Willcox DC, Willcox BJ, Todoriki H, Suzuki M. The Okinawan diet: health implications of a low-calorie, nutrient-dense, antioxidant-rich dietary pattern low in glycemic load. J Am Coll Nutr. 2009;28 Suppl:500S-516S. doi:10.1080/07315724.2009.10718117
- Wright N, Wilson L, Smith M, Duncan B, McHugh P. The BROAD study: A randomised controlled trial using a whole food plant-based diet in the community for obesity, ischaemic heart disease or diabetes. Nutr Diabetes. 2017;7(3):e256. Published 2017 Mar 20. doi:10.1038/nutd.2017.3