
For a long time, we have been told that olive oil is a “superfood.” We see it in commercials and read about it in health magazines. It has a “health halo” around it. It feels like a magic medicine in a bottle. Many people believe that if they just pour more olive oil on their food, their heart will stay healthy forever.
But is this actually true? Does the oil itself have special powers? Or is there a more complicated story happening in our bodies? Recent science suggests that the “magic” might not be in the oil at all. Instead, it might be about what we stop eating when we use olive oil. It is time to look behind the label and see what the science really says.
1. Takeaway 1: It’s Not Magic, It’s “The Swap Effect”
Think about your health like a heavy backpack. Imagine you are hiking and you are carrying a 50-pound backpack made of solid lead. It hurts your back. It makes it very hard to walk. Now, imagine you switch to a 20-pound backpack made of plastic. Your back feels much better! You can walk faster and you don’t feel as tired.
Does this mean the plastic backpack is a “healing” backpack? No. It just means it is less heavy than the lead one.
In science, this is called “replacement dynamics,” but we can just call it The Swap Effect. Big studies from Harvard followed exactly 92,383 people for almost 30 years. They found that people who ate more than half a tablespoon of olive oil a day had about a 19% lower risk of dying from heart disease. That sounds like a big win for olive oil!
However, when the scientists looked closer, they saw the real reason. The people who ate olive oil were usually eating it instead of butter, lard, or margarine. Animal fats are like that heavy lead backpack. They are very hard on the heart. Olive oil is like the lighter plastic backpack. It is a better choice than butter, but that doesn’t mean it is “medicine.”
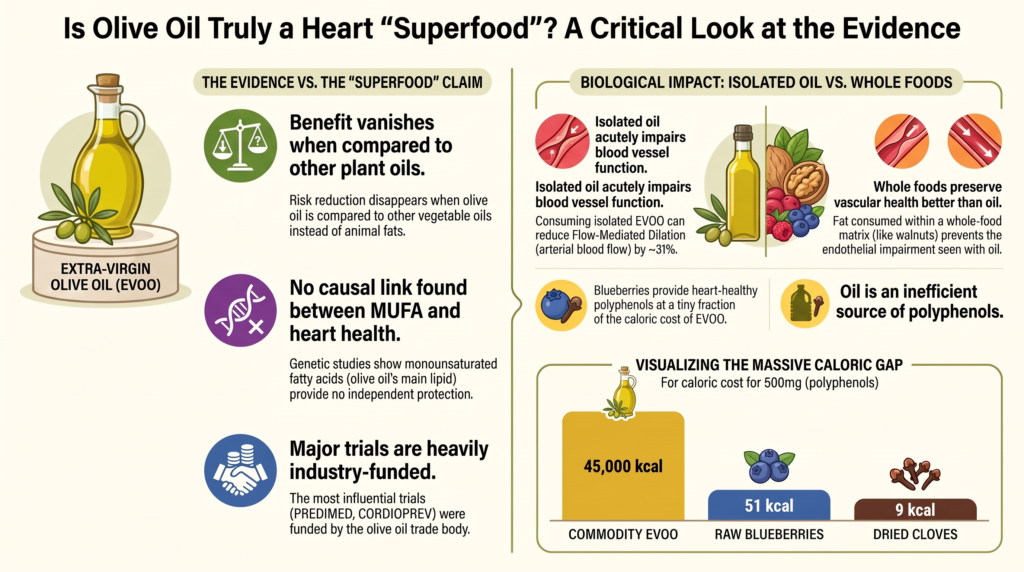
When scientists compared olive oil to other plant oils, the “magic” went away:
- Olive Oil vs. Butter: Olive oil looks like a hero.
- Olive Oil vs. Other Plant Oils (like Soybean or Canola): There was no extra benefit at all.
There was even a big study called a DNA Blueprint Study. This is where scientists look at people who are born with certain genes. They looked at people who naturally had more of the main fat found in olive oil in their blood. If olive oil were magic, these people should have very healthy hearts. But the study found that having more of this fat in your blood did not protect you from heart attacks. This tells us that olive oil is just a “better-than-butter” choice, not a heart-healing star.
2. Takeaway 2: The “Broken” Study and the Money Behind the Bottle
Most of what we think we know about olive oil comes from one very famous study called PREDIMED. But this study had a very big problem.
Imagine you are playing a card game with your friends. For the game to be fair, the deck must be shuffled perfectly. Everyone must have an equal chance to get good cards. In science, we call this “randomization.” But in the PREDIMED study, the “deck” wasn’t shuffled right.
In 2017, an expert named Dr. Carlisle looked at the study and found it was “broken.” About 21% of the people in the study (over 1,500 people) were not put into groups randomly. Here is what went wrong:
- Families put in the same group: Instead of picking individuals, scientists sometimes put whole families into one group together.
- Clinics assigned as a whole: In some cases, a whole doctor’s office was told to eat one way, rather than picking patients one by one.
- Improper use of the random table: The scientists did not follow the rules for how to pick people fairly.
Because of these mistakes, the study had to be retracted. That is like a “do-over” in the science world. It means the results were not as strong as people thought.
We also have to ask who paid for the study. A group called Patrimonio Comunal Olivarero gave the oil and the money for these big trials. This group has one job: to sell more olive oil from Spain. As the science papers say:
“The systematic entanglement of the entire EVOO-efficacy RCT literature with a single interested party is a legitimate basis for caution.”
In simple words: when the people selling the product are the ones paying for the science, we have to be very careful about what we believe.
3. Takeaway 3: The “Garden Hose” Test
To have a healthy heart, your blood vessels need to be flexible. Think of a garden hose. When you turn the water on, the hose needs to be able to stretch to let the water flow through easily. If the hose is stiff and hard, the water can’t get through, and the hose might even crack.
Doctors have a test for this called “Flow-Mediated Dilation” (FMD). It measures how well your “hose” can open up. Scientists did a study where they gave people a meal with olive oil and then tested their blood vessels.
The result was a big warning sign. Just three hours after eating the olive oil, the blood vessels became 31% more stiff. They could not open up nearly as well as they did before the meal.
Why does this happen? When you swallow liquid fat like oil, it rushes into your blood very fast. It creates a “traffic jam” of fat particles. These particles are called chylomicrons. This traffic jam makes the lining of your blood vessels “sticky.”
Here is the “how” of the traffic jam: When the fat enters your blood, it gets chopped into tiny pieces. These pieces are so small that they can “sneak through the cracks” of your blood vessel walls. This is a process called transcytosis. Imagine tiny burglars slipping through a gap in a door. Once they get inside the wall of the vessel, they get stuck. They turn into “sticky messes” that cause inflammation.
However, we must be honest about what this means. While we know the “garden hose” gets stiff for a few hours after eating oil, scientists are not 100% sure yet if this always leads to a heart attack years later. It is a big warning sign, but we are still learning if it is the main cause of long-term damage.
4. Takeaway 4: The 45,000-Calorie Blueberry Challenge
You might hear that olive oil is good because it has “polyphenols.” These are healthy nutrients found in plants. But there is a huge problem with getting your nutrients from oil.
Olive oil is 100% liquid fat. It is very high in calories. One single tablespoon has about 120 calories. To get a healthy amount of polyphenols from a standard bottle of olive oil, you would have to drink a massive amount of it. This is because oil is “naked fat”—it has had all its fiber and most of its nutrients stripped away.
Look at how many calories you would have to eat to get 500mg of these “heart-healthy” nutrients:
| Food Source | Caloric Cost for 500mg of Nutrients |
| Commodity Olive Oil | 45,000 Calories |
| Premium High-Phenolic Oil | 9,000 Calories |
| Dark Chocolate (70%) | 180 Calories |
| Raw Blueberries | 51 Calories |
| Dried Cloves | 9 Calories |
As you can see, trying to get your nutrients from oil is like trying to wash your hands with a fire hose. You get a little bit of what you need, but you get way too much of what you don’t want—thousands of extra calories that can lead to weight gain.
When you eat a whole food like a blueberry, you have a Fiber Shield. The fiber slows down how fast the food enters your blood. This prevents the “traffic jam” in your vessels. Oil has no shield. It hits your blood like a tidal wave.
5. Takeaway 5: Slowing Down vs. Turning Around
There is a big difference between “slowing down” a problem and “fixing” it.
The Mediterranean Diet (which uses olive oil) is better than a standard diet full of butter and meat. It is like driving a car 50 miles per hour toward a cliff instead of 100 miles per hour. You are slowing down the trouble, but you are still heading the wrong way.
On the other hand, a “Whole-Food Plant-Based” (WFPB) diet is different. This diet uses no added oils at all. Instead, people get their healthy fats from whole plants like beans, nuts, and seeds.
Studies by famous doctors like Dr. Ornish and Dr. Esselstyn showed something amazing. When people stopped eating all added oils and switched to whole plants:
- Their “sticky fat particles” (called ApoB) dropped very low. Think of these as the tiny marbles that get stuck in your vessel walls.
- Their “gut bugs” stopped making sticky messes (a chemical called TMAO was markedly reduced).
- Their heart disease actually started to reverse. Their “pipes” started to clear out.
We must be careful here, too. These studies were small, and the people did more than just stop eating oil. They also started exercising, they managed their stress, and they had support groups. This means we can’t say for sure that it was only the oil that made the difference. But it is the only way of eating that has ever shown heart disease can be “turned around” instead of just “slowed down.”
6. Takeaway 6: The Canola Oil Confusion
Many people think the Mediterranean diet is healthy because of olive oil. They point to a famous study called the Lyon Diet Heart Study. In that study, people had a 70% lower risk of heart problems!
But here is the secret: those people were not eating lots of olive oil. Because of a problem in Spain at the time, the scientists actually gave the people a special spread made from canola oil.
This spread had special fats called Omega-3s. These fats are very good at keeping the heart’s rhythm steady. When people say olive oil is the reason for the success of the Mediterranean diet, they are often looking at the wrong oil! This is just another reason to look closely at the facts.
Conclusion: Beyond the Bottle
Olive oil is certainly a better choice than butter or lard. If you are choosing between the two, the oil is the “lighter backpack.” It is a “better-than” choice, but it might not be a “heart-healing” choice.
The real secret to a healthy heart is not found in a bottle of processed, liquid fat. It is found in the whole plant. When we eat the whole olive, the whole walnut, or the whole blueberry, we get the nutrients without the “traffic jam” in our blood. We get the fiber shield that protects our vessels.
The science shows that the best way to protect your heart is to keep those “sticky particles” low and keep your “garden hose” vessels flexible.
If the best science says the secret is in the whole plant, why are we still so focused on the bottle?
DEEP DIVE
Is Olive Oil Independently Cardioprotective?
A Critical Evaluation of Epidemiological, Postprandial, and Clinical Evidence
An evidence-graded review with explicit funding-independence assessment
Abstract
Background. Extra-virgin olive oil (EVOO) is widely promoted as an independently cardioprotective food. This review evaluates whether isolated olive oil has intrinsic cardioprotective properties, separate from the dietary patterns in which it is consumed and from the industry funding that dominates its evidence base.
Methods and scope. Primary peer-reviewed sources (prospective cohorts, randomized controlled trials [RCTs], Mendelian randomization [MR], and controlled postprandial studies) were assessed for their reported effect estimates, evidence grade, and funding independence. Because the olive-oil trade sponsors much of the EVOO efficacy literature, each olive-oil study is explicitly classified as independent or industry-influenced, and residual uncertainty is stated in the text rather than smoothed over.
Findings. Epidemiological associations between olive oil and lower cardiovascular mortality are real but are reproduced in full by other vegetable oils and vanish when olive oil is compared against other plant oils rather than against animal fats. MR finds no causal cardiovascular benefit of circulating monounsaturated fatty acids (MUFAs), the principal olive-oil lipid; the causal signal tracks apolipoprotein B (ApoB) particle number instead. Isolated EVOO acutely impairs endothelial function postprandially, an effect not seen when fat is consumed within a whole-food matrix. Only strict, low-fat, whole-food plant-based (WFPB) patterns excluding all added oils have been shown to arrest and partially reverse angiographic coronary disease. The two major EVOO RCTs (PREDIMED, CORDIOPREV) are both funded by the olive-oil trade body Patrimonio Comunal Olivarero, and PREDIMED was retracted and republished after its randomization was found to be compromised.
Conclusion. Current independent evidence does not demonstrate a clinically meaningful cardioprotective effect of olive oil beyond the replacement of saturated and trans fats; it is best understood as a comparatively benign substitute for animal fat rather than a food with demonstrated unique intrinsic activity. This is a statement about the absence of convincing evidence, not proof of no effect. No large, fully independent hard-outcome RCT of isolated EVOO exists; this evidentiary gap is itself a central finding.
A Note on the Evidence Base and Its Funding
A recurring difficulty in this field is that nearly every RCT purporting to demonstrate EVOO efficacy on cardiovascular endpoints was funded, in cash or in kind, by the olive-oil trade. PREDIMED and CORDIOPREV both received their intervention oil from Patrimonio Comunal Olivarero, an organization whose explicit purpose is to promote Spanish olive-oil exports. [73,76] Industry funding does not by itself invalidate a result, but the systematic entanglement of the entire EVOO-efficacy RCT literature with a single interested party is a legitimate basis for caution. [67,69] Where an independent source supporting the same point exists, it is cited in preference. Where none exists—as is often the case for EVOO—the industry-funded study is retained but flagged in place, and the resulting uncertainty is carried forward into the interpretation. The reader should treat every EVOO efficacy estimate below as provisional to that degree.
1. Epidemiological Quantification of Olive Oil’s Independent Cardioprotective Efficacy
To evaluate whether isolated olive oil possesses independent cardioprotective properties, nutritional epidemiology must be parsed through the lens of replacement dynamics and dietary context. The most comprehensive prospective data in non-Mediterranean cohorts come from the Nurses’ Health Study (NHS) and the Health Professionals Follow-Up Study (HPFS), which together followed 92,383 US men and women free of cardiovascular disease and cancer at baseline for up to 28 years. [1]
Multivariable-adjusted analyses show that individuals in the highest category of olive oil consumption, defined as more than half a tablespoon per day (>7 g/day), exhibited a 19% reduction in cardiovascular mortality (hazard ratio [HR] 0.81; 95% confidence interval [CI] 0.75–0.87) and a 19% reduction in all-cause mortality (HR 0.81; 95% CI 0.78–0.84) versus non-consumers. [1] Higher intake was also associated with an 18% lower risk of coronary heart disease (HR 0.82; 95% CI 0.73–0.91), with no significant association for stroke. [2]
The data further showed a 17% lower risk of cancer mortality (HR 0.83; 95% CI 0.78–0.89), a 29% lower risk of neurodegenerative-disease mortality (HR 0.71; 95% CI 0.64–0.78), and an 18% lower risk of respiratory-disease mortality (HR 0.82; 95% CI 0.72–0.93). [1] A prior draft listed the neurodegenerative CI as 0.78–0.89, which is impossible for a point estimate of 0.71 and in fact belongs to the cancer estimate; the corrected interval is 0.64–0.78.
A separate dose-response meta-analysis of 13 prospective cohorts found each additional 5 g/day of olive oil associated with a small but significant lower risk of CVD (RR 0.96; 95% CI 0.93–0.99) and all-cause mortality (RR 0.96; 95% CI 0.95–0.96). [3] This per-increment figure derives from Xia et al., not the Harvard cohorts, and is attributed accordingly.
The decisive epidemiological test is the head-to-head comparison against other plant oils. Within the same cohorts, replacing 10 g/day of saturated-fat-dense animal lipids (margarine, butter, mayonnaise, dairy fat) with olive oil was associated with an 8% to 34% lower risk of total and cause-specific mortality. [1] But compared directly with other vegetable oils combined, olive oil showed no statistically significant difference for total CVD, CHD, or stroke. [1,2] On these data the apparent benefit tracks the displacement of atherogenic animal fat rather than any intrinsic property of the olive-oil lipid backbone.
Residual confounding compounds this. Those with the highest olive oil intake had healthier lifestyles overall (more physical activity, less smoking, more fruit and vegetables), and the authors acknowledged that high olive oil intake may simply mark higher socioeconomic status and overall diet quality. [1]
1.1 The PREDIMED Primary-Prevention Framework
PREDIMED randomized 7,447 high-risk Spanish adults to a Mediterranean diet plus free EVOO, a Mediterranean diet plus nuts, or a control (low-fat advice) diet, with 4.8 years’ median follow-up. The EVOO arm showed a lower composite rate of myocardial infarction, stroke, and cardiovascular death (HR 0.69; 95% CI 0.53–0.91) versus control, about a 30% relative reduction. [4]
Two caveats weaken this. First, in secondary analyses the inverse association between baseline EVOO intake and hard events held only within the Mediterranean-randomized groups and was abolished in the low-fat control group—so the value of olive oil appears contingent on the surrounding pattern rather than intrinsic. [4]
Second, and more seriously, PREDIMED was retracted. A 2017 reanalysis by Carlisle found baseline distributions statistically incompatible with random allocation. [6] The audit found randomization had failed for ~1,588 of 7,447 participants (~21%): household members assigned en masse at one site; a randomization table not used properly at a second; a clinic randomized as a unit at a third. NEJM retracted the 2013 paper in June 2018 and republished a clustering-adjusted reanalysis. [4,5] As it is no longer strictly individually randomized, PREDIMED is best read as a quasi-randomized intervention; NICE had already judged it at serious risk of bias for individual CVD outcomes. [71]
1.2 Secondary Prevention: CORDIOPREV
CORDIOPREV randomized 1,002 Spanish coronary patients to a Mediterranean diet rich in EVOO (~35% fat, ~22% MUFA) versus a low-fat diet over 7 years. Recurrent MACE occurred at 28.1 per 1,000 person-years (Mediterranean) versus 37.7 per 1,000 person-years (low-fat), multivariable-adjusted hazard ratios across models ranged from 0.719 (95% CI 0.541–0.957) to 0.753 (95% CI 0.568–0.998) in favour of the Mediterranean diet, about a 25–28% relative reduction (log-rank p = 0.039). [8] 28.1 is the Mediterranean-arm incidence rate per 1,000 person-years, not the percent risk reduction; the CI 0.62–0.89 in an earlier draft does not appear in the source and has been replaced with the reported model range.
The comparator was not a genuine low-fat diet. The control group reduced total fat only to ~32% of calories—short of the clinical <30% threshold and far from the <10–15% of the Ornish and Esselstyn reversal trials. Saturated fat was near-identical between arms (~7.9% vs ~7.1%), and the control ate ~10% more protein, mostly animal-source, with fewer legumes, vegetables, and fruits. The benefit may reflect the poor comparator rather than any unique action of EVOO. [8]
A genetic sub-analysis reinforces this: carriers of the ZPR1 rs964184 risk allele on the Mediterranean diet retained elevated fasting and postprandial triglycerides, whereas those on the low-fat diet normalized them—so for certain genotypes the EVOO-rich pattern was inferior for triglyceride clearance. [9]
1.3 Mendelian Randomization: No Causal Signal for MUFA
If oleic acid, the dominant MUFA in olive oil, were directly cardioprotective, genetically higher circulating MUFA should lower risk. Instrumental-variable analyses find no convincing evidence of a causal protective effect of circulating MUFA on CHD, MI, or ischemic stroke. [10] This is a failure to detect an effect rather than positive proof of its absence, but it removes a key plank from the claim of intrinsic benefit. Multivariable MR consistently prioritizes ApoB and LDL particle number as the causal lipid factors, with no independent MUFA signal. [11,12] These genetically anchored, industry-independent data are among the strongest evidence that the cohort associations attributed to olive oil are substantially confounded by consumers’ lifestyle and diet.
Table 1. Key Studies of Olive Oil and Cardiovascular Outcomes
| Study / Cohort | Population & Design | Exposure / Intervention | Effect Estimate (95% CI) | Key Caveats |
| NHS & HPFS mortality [1] | 92,383 US adults; 28-yr prospective cohort | Highest intake (>7 g/day) vs non-consumers | All-cause: HR 0.81 (0.78–0.84) CVD: HR 0.81 (0.75–0.87) |
Benefit fully reproduced by other plant oils; driven by replacing animal fat |
| NHS & HPFS incident CVD [2] | 92,978 US adults; 24-yr prospective cohort | Highest intake vs non-consumers | Total CVD: HR 0.86 (0.79–0.94) CHD: HR 0.82 (0.73–0.91) |
No stroke association; no difference vs other plant oils |
| PREDIMED primary prevention [4] | 7,447 high-risk Spanish adults; 4.8-yr quasi-RCT | MedDiet + EVOO vs low-fat advice | Composite MACE: HR 0.69 (0.53–0.91) | RETRACTED / republished; ~21% mis-randomized; EVOO from olive-oil trade body |
| CORDIOPREV secondary prevention [8] | 1,002 Spanish coronary patients; 7-yr RCT | MedDiet + EVOO vs low-fat diet | Recurrent MACE: HR 0.719–0.753 (e.g., 0.541–0.957) | “Low-fat” control only ~32% fat; funded by olive-oil trade body |
| Mendelian randomization [10–12] | UK Biobank & GWAS meta-analyses | Genetically determined circulating MUFA (oleic acid) | CHD / MI / stroke: no causal association | MUFA not causally protective; ApoB is the causal trait |
Green shading = independent evidence supporting the skeptical thesis. Red shading = industry-funded EVOO efficacy RCTs (retained with caveat; see text).
1.4 The Strongest Case in Favor of Olive Oil
Intellectual honesty requires stating the affirmative case at its strongest before explaining why it falls short of establishing independent efficacy. Several genuine, reproducible findings support olive oil as a component of a heart-healthy pattern.
Saturated-fat replacement and LDL. Substituting olive oil for butter, lard, or other saturated fats lowers LDL cholesterol and ApoB, and the NHS/HPFS substitution analyses show meaningfully lower mortality when olive oil displaces animal fats. [1,65] Because LDL/ApoB is the causal driver of atherosclerosis, this replacement effect is real and clinically useful.
Blood pressure and endothelial markers. Higher-phenolic olive oils have been associated with modest reductions in blood pressure and improvements in some endothelial and inflammatory markers, and the combined phenolic-oil-plus-red-wine data show that context can even produce acute FMD improvement. [16,65] The EFSA-recognized phenolic claim, whatever its practical caloric cost, rests on a genuine in vitro and ex vivo antioxidant signal. [22]
The Mediterranean-pattern signal. Within a whole Mediterranean pattern, EVOO-supplemented diets reduced hard events in both PREDIMED and CORDIOPREV, and reduced carotid plaque progression in CORDIOPREV. [4,8] These are RCT-level outcomes, not merely observational, and they should not be dismissed.
Why this does not establish independent efficacy. Each of these benefits is explicable without invoking a unique property of the olive-oil lipid. The LDL and mortality effects are replacement effects reproduced by other plant oils; the blood-pressure and marker effects are shared by many polyphenol-rich whole foods delivered at far lower caloric cost; the phenolic antioxidant signal has not translated into a phenol-specific in vivo benefit in the cleanest controlled test [24]; and the RCT benefits were measured against weak or animal-protein-rich comparators, within multicomponent patterns, and in trials funded by the olive-oil trade. The affirmative case establishes that olive oil is a good substitute for animal fat and a reasonable part of a plant-rich diet. It does not establish that olive oil, in isolation, is independently cardioprotective—which is the specific claim this review examines.
2. Postprandial Vascular Dynamics: Isolated Oils versus Whole-Food Fats
The acute vascular impact of fat ingestion is seen in the postprandial state—transient endothelial dysfunction, oxidative stress, and inflammatory signaling. The standard index is flow-mediated dilation (FMD) of the brachial artery, a nitric-oxide-dependent response. Consuming isolated dietary oils, including EVOO, consistently produces an acute, significant reduction in FMD. [13]
In a landmark crossover trial, a single 900-kcal meal containing 50 g of fat from isolated olive oil reduced FMD by ~31% at 3 hours, from a baseline of 14.3 ± 4.2% to 9.9 ± 4.5% (p = 0.008); the decline correlated inversely with the postprandial triglyceride rise (r = −0.47, p < 0.05). [13] An earlier draft stated FMD fell “to ~4.5%”; 4.5% is the standard deviation, not the mean. The correct postprandial value is 9.9%, and the trial is Vogel et al. 2000.
Comparative studies show divergence by food matrix: a walnut meal preserves or improves FMD while a fat-matched olive-oil meal worsens it. [14] Caveat: the walnut–oil comparison [14] was funded by the California Walnut Commission and one author served on its Scientific Advisory Board. No fully independent head-to-head walnut-versus-oil postprandial trial was identified, so this result should be read as directionally supportive but industry-influenced.
An essential caveat applies to this entire section. Only the first step of the postulated chain—that isolated oil acutely reduces FMD—has been directly demonstrated. Whether these transient postprandial endothelial impairments translate into accelerated atherosclerosis and, ultimately, into clinical cardiovascular events has not been shown. That progression is biologically plausible and consistent with the response-to-retention framework, but it remains an inference rather than a demonstrated causal sequence in humans. The postprandial data should therefore be read as a mechanistic signal, not as proof of long-term harm from olive oil.
2.1 Mechanism: Chylomicron Remnants and the Response-to-Retention Model
The acute impairment is linked to postprandial lipemia and the response-to-retention model of atherogenesis. [29,33] Rapid absorption of emulsified triacylglycerols from isolated oil produces a surge of chylomicrons; lipoprotein-lipase hydrolysis then yields smaller, atherogenic remnants (<70 nm) that traverse the arterial endothelium via active transcytosis mediated by scavenger receptor class B type 1 (SR-BI) and activin receptor-like kinase 1 (ALK1). [30] Mechanistic (cell/animal and human-biomarker data), not RCT-grade.
In capillaries, this hydrolysis is stabilized by GPIHBP1, which anchors LPL to the luminal surface; larger arteries lack GPIHBP1, so intact remnants interact directly with the arterial wall. [31,32] Retained ApoB-containing remnants bind subendothelial proteoglycans, are oxidized to reactive aldehydes such as 4-hydroxynonenal (4-HNE), and activate NF-κB in endothelium and macrophages, inducing VCAM-1, ICAM-1, and E-selectin; monocytes then adhere, transmigrate, and become foam cells. [33,37,39] Each individual step in this sequence is experimentally supported, but the complete progression from a dietary oil bolus through remnant formation, transcytosis, foam-cell generation, and plaque is inferred by assembling those steps. This integrated pathway remains mechanistic rather than experimentally demonstrated as a continuous sequence in humans.
2.2 Nitric Oxide, ADMA, and eNOS Uncoupling
Postprandial impairment is largely mediated by reduced nitric-oxide bioavailability. Endothelial NO synthase (eNOS) makes NO from L-arginine; asymmetric dimethylarginine (ADMA) competitively inhibits eNOS and is normally cleared by dimethylarginine dimethylaminohydrolase (DDAH). [40,43] During lipemia, ROS and the lipid aldehyde 4-HNE inhibit DDAH, ADMA accumulates, and eNOS uncouples toward superoxide and peroxynitrite, causing acute endothelial dysfunction. [40,41] This is a mechanistically supported model; the dietary-causal specifics are not established by RCT.
2.3 The Whole-Food Matrix Prevents Postprandial Decline
In several controlled studies, whole-food fat sources (fresh avocado, raw walnuts) appear to attenuate or prevent the endothelial impairment seen after isolated oils, rather than reliably eliminating it. [14,15] In a randomized crossover study, substituting fresh Hass avocado for refined carbohydrate improved postprandial FMD and lowered triglyceride-rich lipoproteins versus a fat-matched control. [15] Caveat: avocado postprandial research is frequently funded by the Hass Avocado Board; the specific funding statement should be verified and the result read as industry-adjacent. The intact fiber and cell matrix slow gastric emptying and lipase access, smoothing the triglyceride curve, while co-absorbed antioxidants neutralize ROS, preserve DDAH, and maintain eNOS coupling. [44,47]
The adverse postprandial signature is also modifiable by co-ingested antioxidants. In the Vogel trial, adding vitamins C and E, or a salad with balsamic vinegar, to the olive-oil meal fully prevented the FMD reduction. [13] A separate crossover study reported that combining 50 g of high-phenolic green olive oil with 250 mL of red wine produced a synergistic postprandial FMD improvement sustained for up to two hours (p = 0.002). [16] Funding statement for [16] not retrievable; treat as unverified for independence. Note this result cuts toward “phenolic and whole-food context matters,” not toward isolated-oil benefit. The takeaway is that the endothelial injury of isolated oil is context-dependent, not fixed—but the cleanest way to avoid it is to eat fats in whole-food form.
Table 2. Postprandial Atherogenic Cascade After Isolated-Oil Ingestion (Mechanistic Model)
| Stage | Key Mediators | Mechanism | Effect on eNOS / Permeability |
| 1. Lipemia & remnant generation | Triacylglycerols, chylomicrons, LPL | Rapid absorption of isolated lipid → chylomicron surge; LPL hydrolysis → small dense remnants (<70 nm) | High triglycerides impair systemic vascular reactivity |
| 2. Transcytosis & retention | Remnants, SR-BI, ALK1, proteoglycans | Remnants cross the endothelium via SR-BI/ALK1 and accumulate in the intima | Increased permeability; ApoB particles bind proteoglycans |
| 3. Oxidative modification | ROS, 4-HNE, oxidized remnants | Retained particles are oxidized to cytotoxic aldehydes | 4-HNE inhibits DDAH; eNOS uncouples toward superoxide |
| 4. Endothelial activation | NF-κB, VCAM-1, ICAM-1, E-selectin | Oxidized lipids activate NF-κB → adhesion-molecule expression | Vascular lining becomes adhesive to leukocytes |
| 5. Monocyte recruitment & foam cells | Monocytes, macrophages, scavenger receptors, IL-6, TNF-α | Adhered monocytes transmigrate, differentiate, and form foam cells | Sustained inflammation; loss of vasodilator tone |
This cascade is a mechanistic synthesis of cell, animal, and human-biomarker studies [29–43]; it is not established as an RCT-grade causal chain in humans.
3. Reversal Mechanisms of Whole-Food Plant-Based Diets
Where standard low-fat and Mediterranean patterns generally slow progression, strict low-fat WFPB interventions are the only dietary programs that have demonstrated angiographic regression of coronary disease in published intervention studies. That evidence base is small, highly selected, involves several simultaneous lifestyle changes, and has not been independently replicated at the same scale, and it is described here with those limitations explicit rather than as settled superiority. [54]
Ornish’s Lifestyle Heart Trial (a small RCT, n = 48) combined a ~10%-fat vegetarian diet with no added oils, exercise, stress management, and group support. Quantitative coronary angiography showed regression of average percent-diameter stenosis (40.0% → 37.8% in the intervention group versus progression 42.7% → 46.1% in controls) at 1 year, with further divergence at 5 years. [17,18] LDL cholesterol fell ~37% without lipid-lowering drugs, angina frequency fell markedly, and control patients had roughly twice as many cardiac events by year 5. [18] RCT-grade but small, and the intervention is multi-component, so diet cannot be isolated.
Esselstyn’s case series followed 198 patients with established CVD counseled to a strict WFPB diet excluding all added oils; 177/198 (89%) were adherent. Among adherent patients, one recurrent event occurred (0.6%), versus 13/21 (62%) among the non-adherent, over a mean 3.7 years. [19] Independent (author-declared no conflicts) but uncontrolled, self-selected, and observational—not RCT-grade. The “reversal” claim rests on a small RCT [17,18] plus this uncontrolled cohort; readers should weight it accordingly.
3.1 Direct Clearance of Circulating ApoB
A strict WFPB diet nearly eliminates dietary cholesterol and saturated/trans fat while supplying soluble fiber and phytosterols, depleting hepatic cholesterol pools, activating sterol regulatory element-binding proteins, and upregulating LDL receptors. [48] Circulating ApoB and LDL-C fall, often below 70 mg/dL, reducing the gradient that drives lipoprotein entry into the intima and blunting the initiating step of the response-to-retention cascade. [33,35,36] That ApoB is the causal driver is well established from genetic and clinical data. [35,36]
3.2 Restoration of eNOS Activity and NO Bioavailability
Eliminating added oils and processed fats lowers triglycerides and prevents ADMA-mediated eNOS uncoupling; leafy greens supply inorganic nitrate reduced to nitrite and then bioactive NO; and abundant polyphenols protect tetrahydrobiopterin (BH4), keeping eNOS coupled. [43,50] These are mechanistically supported pathways rather than hard clinical endpoints.
3.3 The TMAO Pathway
Trimethylamine-N-oxide (TMAO), a gut-microbiota-dependent metabolite of dietary carnitine and choline, is associated with accelerated atherosclerosis via effects on macrophage scavenger receptors and reverse cholesterol transport. [52,53] A WFPB shift enriches fiber-fermenting taxa and depletes TMA-producing species, markedly reducing TMAO production. [53] An earlier draft said WFPB “entirely abolishes” TMAO; this overreaches. Vegans produce far less TMAO after a carnitine challenge, but endogenous choline metabolism and residual microbial activity mean TMAO is reduced, not eliminated. The claim is corrected to “markedly reduces.”
3.4 Attenuation of Systemic Inflammation
Fiber fermentation yields short-chain fatty acids that lower systemic inflammation; WFPB patterns reduce high-sensitivity C-reactive protein and downregulate NF-κB-driven adhesion-molecule expression, shifting the arterial wall from active recruitment toward resolution. [54,62] Effect sizes vary across small trials and should not be over-stated.
Table 3. Comparative Effects of Three Dietary Patterns
| Parameter | Low-Fat Control (30–35% fat) | Mediterranean + EVOO | Strict No-Added-Oil WFPB |
| LDL-C / ApoB | Minimal-to-modest reductions; often fails to lower ApoB to physiological range | Modest reductions; LDL-C typically remains 80–100 mg/dL, leaving residual particle risk | Profound reductions; frequently LDL-C <70 mg/dL, minimizing intimal entry |
| Postprandial FMD / NO | Transient impairment from refined carbohydrate or saturated fat | Acute FMD reduction (~31% in [13]) unless paired with antioxidants | Postprandial FMD preserved; no added oil, high NO bioavailability |
| Systemic inflammation (hs-CRP) | Minimal reduction | Significant reduction reported (industry-linked trials; caveat applies) | Substantial reduction; NF-κB downregulated |
| Plaque progression | Continued progression even with statins | Delayed progression; slight IMT regression; recurrent events persist | Documented angiographic arrest and partial regression (small studies) |
| Microbial TMAO | High; ongoing conversion of carnitine/choline | Variable; persists with fish, poultry, dairy | Markedly reduced (not fully abolished) |
Estimates for the Mediterranean and WFPB columns derive from trials of differing size and funding independence; see text and Section 4 for caveats.
4. Deconstruction of Industry Sponsorship and Nutritional Claims
4.1 The PREDIMED Retraction and Randomization Failures
PREDIMED, published in NEJM in 2013, was the most influential trial supporting the Mediterranean diet and EVOO. [68] Carlisle’s 2017 reanalysis found baseline distributions incompatible with randomization (p < 0.0001). [6] The internal audit found systemic departures from randomization affecting ~1,588 participants (~21% of the cohort): en-masse household assignment at one site, improper use of the randomization table at another, and clinic-level (rather than individual) assignment at a third. [4,5] NEJM retracted the 2013 paper in June 2018 and republished a reanalysis; because it was no longer strictly randomized, its evidence grade fell to that of a quasi-randomized cohort-style intervention. NICE had assessed it at serious risk of bias with low-to-very-low-quality data for individual outcomes. [71]
4.2 CORDIOPREV: A Weak Comparator
CORDIOPREV is cited as the premier secondary-prevention trial favoring a Mediterranean over a low-fat diet, but its control arm did not reach a genuine low-fat target (~32% of calories from fat, versus the <30% clinical definition and the <10–15% of Ornish and Esselstyn). [8] Saturated fat was near-identical between arms, and the control consumed ~10% more protein—mostly animal-source—while eating fewer whole plant foods. The ~26% MACE reduction may reflect the poor control diet rather than any unique EVOO mechanism. [8]
4.3 Funding Sources and Conflicts of Interest
The two major hard-outcome EVOO RCTs discussed here are PREDIMED and CORDIOPREV; numerous smaller RCTs of olive oil on surrogate markers also exist, but none tests hard cardiovascular endpoints independently of the olive-oil trade. PREDIMED, though primarily government-funded, received donated EVOO from Hojiblanca and Patrimonio Comunal Olivarero, and donated nuts from the California Walnut Commission and others. [73] Disclosed steering-committee conflicts include Emilio Ros (research grants from and Scientific Advisory Committee membership of the California Walnut Commission) and Jordi Salas-Salvadó (grants from and unpaid advisory membership of the International Nut and Dried Fruit Council). [74] An earlier draft attributed International Nut Council funding to M. Á. Martínez-González; that attribution is not supported by the disclosures and has been removed. The verified nut-industry tie belongs to Salas-Salvadó.
CORDIOPREV was supported by the Fundación Patrimonio Comunal Olivarero, an organization dedicated to promoting Spanish olive-oil exports; its very acronym encodes the sponsor’s interest. [76] These systematic ties between a single trade interest and the entire EVOO-efficacy RCT literature justify treating “olive oil as superfood” framing with caution. [67,69]
4.4 The Lyon Diet Heart Study: Canola, Not Olive Oil
The Lyon Diet Heart Study is often invoked for Mediterranean secondary prevention, reporting roughly a 70% lower all-cause mortality (adjusted risk ratio 0.30; 95% CI 0.11–0.82). [27,28] But its supplemental fat was not olive oil: the experimental group received a custom canola-oil-based margarine designed to mimic a Cretan profile, high in alpha-linolenic acid (ALA), with a low omega-6:omega-3 ratio (~2.8). [27,79] Reviewers attributed the mortality benefit substantially to ALA’s anti-arrhythmic and anti-thrombotic effects rather than to olive oil. [78] The choice of canola reflected, in part, Spain’s Toxic Oil Syndrome history, which had made rapeseed-oil trials socially fraught there; this is historical context, not a cardioprotection claim.
4.5 The Polyphenol “Health Halo” and the Caloric-Efficiency Gap
A central marketing claim is EVOO’s biophenol content (hydroxytyrosol, oleuropein, oleocanthal, oleacein). In 2011 the European Food Safety Authority approved a claim that olive-oil polyphenols protect blood lipids from oxidative stress, conditional on ≥5 mg of hydroxytyrosol and its derivatives per 20 g of oil, at 20 g/day. [22,23]
But olive oil is a calorically expensive polyphenol vehicle. It is ~100% lipid (~900 kcal/100 g, ~120 kcal per tablespoon) with negligible fiber, protein, or water-soluble micronutrients. [47] Commodity EVOO often falls below the EFSA threshold, and even premium high-phenolic oils require large lipid loads to deliver a meaningful polyphenol dose, whereas whole plant foods deliver far more polyphenol per calorie. [21,85] The per-food polyphenol values below trace to the Phenol-Explorer database and vary with assay and extraction; the derived gram/calorie figures are illustrative arithmetic, not measured trial outcomes.
Table 4. Caloric Cost of Obtaining 500 mg of Polyphenols by Food Source
| Food Source | Polyphenols (mg/100 g) | Energy (kcal/100 g) | Mass for 500 mg (g) | Caloric cost (kcal) |
| Commodity EVOO | ~10 | 900 | 5,000 | 45,000 |
| Premium high-phenolic EVOO | ~50 | 900 | 1,000 | 9,000 |
| Raw blueberries | 560 | 57 | 89 | 51 |
| Black chokeberries | 1,022 | 47 | 49 | 23 |
| Dark chocolate (≥70%) | 1,664 | 598 | 30 | 180 |
| Dried cloves | 15,188 | 274 | 3.3 | 9 |
Polyphenol concentrations from Phenol-Explorer [21,85]; energy values from USDA. Red = calorically expensive polyphenol vehicles; green = efficient whole-food sources. Values should be verified per cell before publication, as Folin assay results vary by method.
4.6 Do the Phenolics Deliver In Vivo?
A controlled crossover trial found that olive oil fortified with polar or non-polar phenolics increased LDL-oxidation lag time by ~8 minutes—but the same increase occurred with the polyphenol-free placebo oil, suggesting a non-specific meal or time effect rather than a unique phenolic benefit. [24] A single trial cannot overturn a field, and other work reports phenol-specific effects; but this relatively independent (Wageningen-led) study raises important questions about the magnitude of the proposed antioxidant mechanism and cautions against treating it as established. [24] Related LDL-oxidation analyses by the same group had Unilever affiliation or International Olive Oil Council funding [89]; the specifically cited 2001 Free Radical Research paper [24] is the cleaner source and is used here.
Some industry-linked trials (e.g., EUROLIVE and HDL-function studies) do report phenolic benefits. [49,86] These are cited for completeness but carry funding caveats and should not be read as independent confirmation. [61,63]
The pharmacology of oleocanthal is real but distinct from clinical cardioprotection: it inhibits COX-1 and COX-2 dose-dependently, like ibuprofen, [25] while the peppery throat sting of high-phenolic oil is mediated by TRPA1 channels restricted to the posterior oropharynx—a sensory phenomenon with no established bearing on cardiovascular outcomes. [26]
5. Conclusions
A critical synthesis indicates that current independent evidence does not demonstrate a clinically meaningful cardioprotective effect of isolated olive oil beyond the replacement of saturated and trans fats. This is a conclusion about the absence of convincing evidence for unique benefit, not positive proof that no such benefit exists. Epidemiological associations are real but are reproduced by other plant oils and are consistent with the displacement of animal fat; MR finds no convincing evidence of a causal MUFA effect and points instead to ApoB. [1,2,10,11]
Physiologically, isolated EVOO acutely impairs postprandial endothelial function by accelerating chylomicron-remnant generation and retention—an effect that whole-food fat sources appear to attenuate. Whether this transient postprandial impairment translates into long-term atherosclerosis and clinical events has not been demonstrated; it is a plausible mechanistic link, not an established one, and should be presented as such. [13,14,15]
While EVOO-supplemented diets can slow progression relative to weak comparators, only strict low-fat WFPB patterns excluding added oils have been shown to arrest and partially reverse angiographic coronary disease—though that evidence rests on one small RCT and an uncontrolled cohort and should be described with appropriate humility. [17,18,19]
Finally, the EVOO efficacy literature is systematically entangled with the olive-oil trade, and its most influential trial was retracted for randomization failure. The strongest evidence in this review—the null comparison against other plant oils, the null MUFA MR, and the null phenolic LDL-oxidation trial—comes from independent or government-funded work. [1,10,24]
The central evidentiary gap: no large, fully independent RCT of isolated EVOO on hard cardiovascular endpoints exists. Until one does, claims of unique olive-oil cardioprotection should be regarded as unproven, and the reader is entitled to the residual doubt that this review has tried to make explicit throughout.
References
Citations follow IEEE style and are numbered in order of first appearance. Primary peer-reviewed sources (PubMed/PMC) are used throughout; entries marked “mechanistic” denote preclinical or biomarker-level evidence rather than RCT-grade clinical outcomes. Funding caveats for industry-linked olive-oil sources are noted in the text.
-
- Guasch-Ferré M, Li Y, Willett WC, et al. Consumption of Olive Oil and Risk of Total and Cause-Specific Mortality Among U.S. Adults. J Am Coll Cardiol. 2022;79(2):101-112. doi:10.1016/j.jacc.2021.10.041
- Guasch-Ferré M, Liu G, Li Y, et al. Olive Oil Consumption and Cardiovascular Risk in U.S. Adults. J Am Coll Cardiol. 2020;75(15):1729-1739. doi:10.1016/j.jacc.2020.02.036
- Xia M, Zhong Y, Peng Y, Qian C. Olive oil consumption and risk of cardiovascular disease and all-cause mortality: A meta-analysis of prospective cohort studies. Front Nutr. 2022;9:1041203. Published 2022 Oct 18. doi:10.3389/fnut.2022.1041203
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389
- Estruch R, Ros E, Salas-Salvadó J, et al. Retraction and Republication: Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med 2013;368:1279-90 [retraction of: N Engl J Med. 2013 Apr 4;368(14):1279-90. doi: 10.1056/NEJMoa1200303.]. N Engl J Med. 2018;378(25):2441-2442. doi:10.1056/NEJMc1806491
- Carlisle JB. Data fabrication and other reasons for non-random sampling in 5087 randomised, controlled trials in anaesthetic and general medical journals. Anaesthesia. 2017;72(8):944-952. doi:10.1111/anae.13938
- Martínez-González MÁ, Toledo E, Arós F, et al. Extravirgin olive oil consumption reduces risk of atrial fibrillation: the PREDIMED (Prevención con Dieta Mediterránea) trial. Circulation. 2014;130(1):18-26. doi:10.1161/CIRCULATIONAHA.113.006921
- Delgado-Lista J, Alcala-Diaz JF, Torres-Peña JD, et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. Lancet. 2022;399(10338):1876-1885. doi:10.1016/S0140-6736(22)00122-2
- Alcala-Diaz JF, Arenas-de Larriva AP, Torres-Peña JD, et al. A Gene Variation at the ZPR1 Locus (rs964184) Interacts With the Type of Diet to Modulate Postprandial Triglycerides in Patients With Coronary Artery Disease: From the Coronary Diet Intervention With Olive Oil and Cardiovascular Prevention Study. Front Nutr. 2022;9:885256. Published 2022 Jun 17. doi:10.3389/fnut.2022.885256
- Mazidi M, Katsiki N, Shekoohi N, Banach M. Monounsaturated Fatty Acid Levels May Not Affect Cardiovascular Events: Results From a Mendelian Randomization Analysis. Front Nutr. 2020;7:123. Published 2020 Sep 2. doi:10.3389/fnut.2020.00123
- Zagkos L, Dib MJ, Pinto R, et al. Associations of genetically predicted fatty acid levels across the phenome: A mendelian randomisation study. PLoS Med. 2022;19(12):e1004141. Published 2022 Dec 29. doi:10.1371/journal.pmed.1004141
- Richardson TG, Sanderson E, Palmer TM, et al. Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis. PLoS Med. 2020;17(3):e1003062. Published 2020 Mar 23. doi:10.1371/journal.pmed.1003062
- Vogel RA, Corretti MC, Plotnick GD. The postprandial effect of components of the Mediterranean diet on endothelial function. J Am Coll Cardiol. 2000;36(5):1455-1460. doi:10.1016/s0735-1097(00)00896-2
- Cortés B, Núñez I, Cofán M, et al. Acute effects of high-fat meals enriched with walnuts or olive oil on postprandial endothelial function. J Am Coll Cardiol. 2006;48(8):1666-1671. doi:10.1016/j.jacc.2006.06.057
- Wang L, Bordi PL, Fleming JA, Hill AM, Kris-Etherton PM. Effect of a moderate fat diet with and without avocados on lipoprotein particle number, size and subclasses in overweight and obese adults: a randomized, controlled trial. J Am Heart Assoc. 2015;4(1):e001355. Published 2015 Jan 7. doi:10.1161/JAHA.114.001355
- Karatzi K, Papamichael C, Karatzis E, et al. Postprandial improvement of endothelial function by red wine and olive oil antioxidants: a synergistic effect of components of the Mediterranean diet. J Am Coll Nutr. 2008;27(4):448-453. doi:10.1080/07315724.2008.10719724
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336(8708):129-133. doi:10.1016/0140-6736(90)91656-u
- Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001-2007. doi:10.1001/jama.280.23.2001
- Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD?. J Fam Pract. 2014;63(7):356-364b.
- Esselstyn CB Jr. Updating a 12-year experience with arrest and reversal therapy for coronary heart disease (an overdue requiem for palliative cardiology). Am J Cardiol. 1999;84(3):339-A8. doi:10.1016/s0002-9149(99)00290-8
- Pérez-Jiménez J, Neveu V, Vos F, Scalbert A. Identification of the 100 richest dietary sources of polyphenols: an application of the Phenol-Explorer database. Eur J Clin Nutr. 2010;64 Suppl 3:S112-S120. doi:10.1038/ejcn.2010.221
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to polyphenols in olive and protection of LDL particles from oxidative damage (ID 1333, 1638, 1639, 1696, 2865), maintenance of normal blood HDL cholesterol concentrations (ID 1639), maintenance of normal blood pressure (ID 3781), “anti-inflammatory properties” (ID 1882), “contributes to the upper respiratory tract health” (ID 3468), “can help to maintain a normal function of gastrointestinal tract” (3779), and “contributes to body defences against external agents” (ID 3467) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2011;9(4):2033. Published 2011 Apr 8. doi:10.2903/j.efsa.2011.2033
- Commission Regulation (EU) No 432/2012 of 16 May 2012 establishing a list of permitted health claims made on foods, Off. J. Eur. Union, L 136, pp. 1–40, May 2012.
- Vissers MN, Zock PL, Leenen R, Roodenburg AJ, van Putte KP, Katan MB. Effect of consumption of phenols from olives and extra virgin olive oil on LDL oxidizability in healthy humans. Free Radic Res. 2001;35(5):619-629. doi:10.1080/10715760100301621
- Beauchamp GK, Keast RS, Morel D, et al. Phytochemistry: ibuprofen-like activity in extra-virgin olive oil. Nature. 2005;437(7055):45-46. doi:10.1038/437045a
- Peyrot des Gachons C, Uchida K, Bryant B, et al. Unusual pungency from extra-virgin olive oil is attributable to restricted spatial expression of the receptor of oleocanthal. J Neurosci. 2011;31(3):999-1009. doi:10.1523/JNEUROSCI.1374-10.2011
- de Lorgeril M, Renaud S, Mamelle N, et al. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet. 1994;343(8911):1454-1459. doi:10.1016/s0140-6736(94)92580-1
- de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation. 1999;99(6):779-785. doi:10.1161/01.cir.99.6.779
- Williams KJ, Tabas I. The response-to-retention hypothesis of early atherogenesis. Arterioscler Thromb Vasc Biol. 1995;15(5):551-561. doi:10.1161/01.atv.15.5.551
- Bolanle IO, de Liedekerke Beaufort GC, Weinberg PD. Transcytosis of LDL Across Arterial Endothelium: Mechanisms and Therapeutic Targets. Arterioscler Thromb Vasc Biol. 2025;45(4):468-480. doi:10.1161/ATVBAHA.124.321549
- Beigneux AP. GPIHBP1 and the processing of triglyceride-rich lipoproteins. Clin Lipidol. 2010;5(4):575-582. doi:10.2217/clp.10.43
- Goldberg IJ, Bornfeldt KE. Lipids and the endothelium: bidirectional interactions. Curr Atheroscler Rep. 2013;15(11):365. doi:10.1007/s11883-013-0365-1
- Tabas I, Williams KJ, Borén J. Subendothelial lipoprotein retention as the initiating process in atherosclerosis: update and therapeutic implications. Circulation. 2007;116(16):1832-1844. doi:10.1161/CIRCULATIONAHA.106.676890
- Badimon L, Vilahur G. LDL-cholesterol versus HDL-cholesterol in the atherosclerotic plaque: inflammatory resolution versus thrombotic chaos. Ann N Y Acad Sci. 2012;1254:18-32. doi:10.1111/j.1749-6632.2012.06480.x
- Borén J, Chapman MJ, Krauss RM, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2020;41(24):2313-2330. doi:10.1093/eurheartj/ehz962
- Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2017;38(32):2459-2472. doi:10.1093/eurheartj/ehx144
- Libby P. The changing landscape of atherosclerosis. Nature. 2021;592(7855):524-533. doi:10.1038/s41586-021-03392-8
- van Oostrom AJ, Rabelink TJ, Verseyden C, et al. Activation of leukocytes by postprandial lipemia in healthy volunteers. Atherosclerosis. 2004;177(1):175-182. doi:10.1016/j.atherosclerosis.2004.07.004
- Tsimikas S, Witztum JL. Oxidized phospholipids in cardiovascular disease. Nat Rev Cardiol. 2024;21(3):170-191. doi:10.1038/s41569-023-00937-4
- Böger RH. The emerging role of asymmetric dimethylarginine as a novel cardiovascular risk factor. Cardiovasc Res. 2003;59(4):824-833. doi:10.1016/s0008-6363(03)00500-5
- Böger RH. Asymmetric dimethylarginine (ADMA): a novel risk marker in cardiovascular medicine and beyond. Ann Med. 2006;38(2):126-136. doi:10.1080/07853890500472151
- Zhao G, Etherton TD, Martin KR, Gillies PJ, West SG, Kris-Etherton PM. Dietary alpha-linolenic acid inhibits proinflammatory cytokine production by peripheral blood mononuclear cells in hypercholesterolemic subjects. Am J Clin Nutr. 2007;85(2):385-391. doi:10.1093/ajcn/85.2.385
- Förstermann U, Sessa WC. Nitric oxide synthases: regulation and function. Eur Heart J. 2012;33(7):829-837d. doi:10.1093/eurheartj/ehr304
- Kris-Etherton PM, Hecker KD, Bonanome A, et al. Bioactive compounds in foods: their role in the prevention of cardiovascular disease and cancer. Am J Med. 2002;113 Suppl 9B:71S-88S. doi:10.1016/s0002-9343(01)00995-0
- Ornish D. Avoiding revascularization with lifestyle changes: The Multicenter Lifestyle Demonstration Project. Am J Cardiol. 1998;82(10B):72T-76T. doi:10.1016/s0002-9149(98)00744-9
- Dreher ML, Davenport AJ. Hass avocado composition and potential health effects. Crit Rev Food Sci Nutr. 2013;53(7):738-750. doi:10.1080/10408398.2011.556759
- Rajaram S. The effect of vegetarian diet, plant foods, and phytochemicals on hemostasis and thrombosis. Am J Clin Nutr. 2003;78(3 Suppl):552S-558S. doi:10.1093/ajcn/78.3.552S
- Jenkins DJ, Kendall CW, Marchie A, et al. Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-reactive protein. JAMA. 2003;290(4):502-510. doi:10.1001/jama.290.4.502
- Covas MI, Nyyssönen K, Poulsen HE, et al. The effect of polyphenols in olive oil on heart disease risk factors: a randomized trial. Ann Intern Med. 2006;145(5):333-341. doi:10.7326/0003-4819-145-5-200609050-00006
- Kapil V, Khambata RS, Robertson A, Caulfield MJ, Ahluwalia A. Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: a randomized, phase 2, double-blind, placebo-controlled study. Hypertension. 2015;65(2):320-327. doi:10.1161/HYPERTENSIONAHA.114.04675
- Karatzi K, Papamichael C, Karatzis E, et al. Postprandial improvement of endothelial function by red wine and olive oil antioxidants: a synergistic effect of components of the Mediterranean diet. J Am Coll Nutr. 2008;27(4):448-453. doi:10.1080/07315724.2008.10719724
- Tang WH, Wang Z, Levison BS, et al. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013;368(17):1575-1584. doi:10.1056/NEJMoa1109400
- Koeth RA, Wang Z, Levison BS, et al. Intestinal microbiota metabolism of L-carnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med. 2013;19(5):576-585. doi:10.1038/nm.3145
- Tuso P, Stoll SR, Li WW. A plant-based diet, atherogenesis, and coronary artery disease prevention. Perm J. 2015;19(1):62-67. doi:10.7812/TPP/14-036
- Esselstyn CB. A plant-based diet and coronary artery disease: a mandate for effective therapy. J Geriatr Cardiol. 2017;14(5):317-320. doi:10.11909/j.issn.1671-5411.2017.05.004
- Esselstyn CB Jr, Ellis SG, Medendorp SV, Crowe TD. A strategy to arrest and reverse coronary artery disease: a 5-year longitudinal study of a single physician’s practice. J Fam Pract. 1995;41(6):560-568.
- Fernández-Rodríguez R, Bizzozero-Peroni B, Díaz-Goñi V, et al. Plant-based meat alternatives and cardiometabolic health: a systematic review and meta-analysis. Am J Clin Nutr. 2025;121(2):274-283. doi:10.1016/j.ajcnut.2024.12.002
- Campbell TC. A plant-based diet and animal protein: questioning dietary fat and considering animal protein as the main cause of heart disease. J Geriatr Cardiol. 2017;14(5):331-337. doi:10.11909/j.issn.1671-5411.2017.05.011
- Dinu M, Abbate R, Gensini GF, Casini A, Sofi F. Vegetarian, vegan diets and multiple health outcomes: A systematic review with meta-analysis of observational studies. Crit Rev Food Sci Nutr. 2017;57(17):3640-3649. doi:10.1080/10408398.2016.1138447
- Weech M, Altowaijri H, Mayneris-Perxachs J, et al. Replacement of dietary saturated fat with unsaturated fats increases numbers of circulating endothelial progenitor cells and decreases numbers of microparticles: findings from the randomized, controlled Dietary Intervention and VAScular function (DIVAS) study. Am J Clin Nutr. 2018;107(6):876-882. doi:10.1093/ajcn/nqy018
- M.-I. Covas et al., “Minor components of olive oil: Evidence to date of health benefits in humans,” Nutr. Rev., vol. 64, no. 10 pt 2, pp. S20–S30, 2006 (industry-linked review; funding caveat in text).
- Kahleova H, Levin S, Barnard N. Cardio-Metabolic Benefits of Plant-Based Diets. Nutrients. 2017;9(8):848. Published 2017 Aug 9. doi:10.3390/nu9080848
- Estruch R. Anti-inflammatory effects of the Mediterranean diet: the experience of the PREDIMED study. Proc Nutr Soc. 2010;69(3):333-340. doi:10.1017/S0029665110001539
- Nishi SK, Paz-Graniel I, Ni J, et al. Effect of nut consumption on blood lipids: An updated systematic review and meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2025;35(5):103771. doi:10.1016/j.numecd.2024.10.009
- Schwingshackl L, Hoffmann G. Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies. Lipids Health Dis. 2014;13:154. Published 2014 Oct 1. doi:10.1186/1476-511X-13-154
- Ros E, Martínez-González MA, Estruch R, et al. Mediterranean diet and cardiovascular health: Teachings of the PREDIMED study. Adv Nutr. 2014;5(3):330S-6S. Published 2014 May 14. doi:10.3945/an.113.005389
- Nestle M. Food Industry Funding of Nutrition Research: The Relevance of History for Current Debates. JAMA Intern Med. 2016;176(11):1685-1686. doi:10.1001/jamainternmed.2016.5400
- Estruch R, Ros E, Salas-Salvadó J, et al. Retraction and Republication: Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N Engl J Med 2013;368:1279-90 [retraction of: N Engl J Med. 2013 Apr 4;368(14):1279-90. doi: 10.1056/NEJMoa1200303.]. N Engl J Med. 2018;378(25):2441-2442. doi:10.1056/NEJMc1806491
- Bero L. Industry sponsorship and research outcome: a Cochrane review. JAMA Intern Med. 2013;173(7):580-581. doi:10.1001/jamainternmed.2013.4190
- A.-M. Chang et al., commentary on PREDIMED randomization irregularities, republished analysis context, N. Engl. J. Med., 2018 (see [4], [5]).
- Evidence review for dietary cholesterol strategies: Cardiovascular disease: risk assessment and reduction, including lipid modification. London: National Institute for Health and Care Excellence (NICE); May 2023.
- Alcala-Diaz JF, Arenas-de Larriva AP, Torres-Peña JD, et al. A Gene Variation at the ZPR1 Locus (rs964184) Interacts With the Type of Diet to Modulate Postprandial Triglycerides in Patients With Coronary Artery Disease: From the Coronary Diet Intervention With Olive Oil and Cardiovascular Prevention Study. Front Nutr. 2022;9:885256. Published 2022 Jun 17. doi:10.3389/fnut.2022.885256
- PREDIMED Study Investigators, “Funding and food-industry donations disclosure,” in [4] supplementary appendix, N. Engl. J. Med., 2018.
- Conflict-of-interest disclosures, PREDIMED steering committee, in [4] supplementary appendix (E. Ros: California Walnut Commission; J. Salas-Salvadó: International Nut and Dried Fruit Council), N. Engl. J. Med., 2018.
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389
- Fundación Patrimonio Comunal Olivarero, funding acknowledgment, in CORDIOPREV [8], Lancet, 2022.
- de Lorgeril M, Salen P. The Mediterranean diet in secondary prevention of coronary heart disease. Clin Invest Med. 2006;29(3):154-158.
- Visioli F, Galli C. Alpha-linolenic acid and cardiovascular disease. Am J Clin Nutr. 2002;75(6):1121-1122. doi:10.1093/ajcn/75.6.1121
- de Lorgeril M, Salen P. Modified Cretan Mediterranean diet in the prevention of coronary heart disease and cancer. World Rev Nutr Diet. 2000;87:1-23.
- Hu FB. The Mediterranean diet and mortality–olive oil and beyond. N Engl J Med. 2003;348(26):2595-2596. doi:10.1056/NEJMp030069
- EFSA Panel on Nutrition, Novel Foods and Food allergens (NDA), Turck D, Bohn T, et al. Olive oil polyphenols and the maintenance of normal HDL-cholesterol concentrations: Evaluation of a health claim pursuant to Article 13(5) of Regulation (EC) No 1924/2006. EFSA J. 2025;23(5):e9372. Published 2025 May 2. doi:10.2903/j.efsa.2025.9372
- Fabiani R. Anti-cancer properties of olive oil secoiridoid phenols: a systematic review of in vivo studies. Food Funct. 2016;7(10):4145-4159. doi:10.1039/c6fo00958a
- Owen RW, Giacosa A, Hull WE, et al. Olive-oil consumption and health: the possible role of antioxidants. Lancet Oncol. 2000;1:107-112. doi:10.1016/s1470-2045(00)00015-2
- Crespo MC, Tomé-Carneiro J, Dávalos A, Visioli F. Pharma-Nutritional Properties of Olive Oil Phenols. Transfer of New Findings to Human Nutrition. Foods. 2018;7(6):90. Published 2018 Jun 11. doi:10.3390/foods7060090
- Neveu V, Perez-Jiménez J, Vos F, et al. Phenol-Explorer: an online comprehensive database on polyphenol contents in foods. Database (Oxford). 2010;2010:bap024. doi:10.1093/database/bap024
- Hernáez Á, Fernández-Castillejo S, Farràs M, et al. Olive oil polyphenols enhance high-density lipoprotein function in humans: a randomized controlled trial. Arterioscler Thromb Vasc Biol. 2014;34(9):2115-2119. doi:10.1161/ATVBAHA.114.303374
- Key TJ, Fraser GE, Thorogood M, et al. Mortality in vegetarians and nonvegetarians: detailed findings from a collaborative analysis of 5 prospective studies. Am J Clin Nutr. 1999;70(3 Suppl):516S-524S. doi:10.1093/ajcn/70.3.516s
- Yeung AWK. Food Composition Databases (FCDBs): A Bibliometric Analysis. Nutrients. 2023;15(16):3548. Published 2023 Aug 11. doi:10.3390/nu15163548
- Castañer O, Covas MI, Khymenets O, et al. Protection of LDL from oxidation by olive oil polyphenols is associated with a downregulation of CD40-ligand expression and its downstream products in vivo in humans. Am J Clin Nutr. 2012;95(5):1238-1244. doi:10.3945/ajcn.111.029207