
Are High Cardiac Calcium Scores Bad for Endurance Athletes?
The Athlete Paradox: The Clinical Paradigm of Coronary Artery Calcium: Assessing Risk in Asymptomatic Populations
The landscape of preventive cardiology has undergone a profound transformation with the emergence of subclinical imaging, specifically the quantification of coronary artery calcium (CAC). For decades, cardiovascular risk assessment relied almost exclusively on probabilistic models derived from population-wide observational data. While tools such as the Framingham Risk Score and the Pooled Cohort Equations have provided a foundation for primary prevention, they remain indirect measures of risk, estimating the likelihood of disease based on surrogate markers like cholesterol levels and blood pressure. The integration of CAC scoring into clinical practice represents a shift toward a disease-based approach, where the direct visualization of atherosclerotic burden allows for highly individualized risk stratification. In the general population, the presence and extent of coronary calcium is a robust and independent predictor of future myocardial infarction and cardiovascular mortality.¹ However, a growing body of evidence has identified a counterintuitive phenomenon in masters endurance athletes: these individuals, who often possess superior cardiorespiratory fitness and lower overall mortality, frequently exhibit higher CAC scores and more coronary plaque than their sedentary peers.² This report explores the technical underpinnings of CAC scoring, its predictive performance in the general population, the biological mechanisms proposed to explain the athletic paradox, and its comparative utility against other modern risk prediction tools.
Technical Foundations of Coronary Artery Calcium Scoring
Coronary artery calcium (CAC) is a highly specific marker of coronary atherosclerosis and a practical surrogate for overall coronary plaque burden.¹,³ The development of calcified plaque in the coronary arteries is an active, regulated biological process rather than a passive accumulation of minerals. It typically reflects more advanced phases of the atherosclerotic cascade and correlates with total plaque burden in the epicardial coronary arteries.¹,³ Because calcification reflects only a portion of total atherosclerosis, the presence of detectable calcium generally implies a larger underlying burden that can include both calcified and non-calcified atheroma.¹,³
Mechanics of Computed Tomography and the Agatston Method
The standard method for assessing coronary calcium is through non-contrast, electrocardiogram (ECG)-gated computed tomography (CT) of the chest. To ensure high-quality imaging and minimize motion artifacts from the cardiac cycle, scans are typically acquired during a single breath-hold using prospective ECG triggering.³ This synchronization allows the scanner to capture images primarily during diastole, when the heart is most still.³ Modern multidetector computed tomography (MDCT) systems have largely replaced earlier electron beam computed tomography (EBCT) due to their widespread availability and high spatial resolution.³
The quantification of coronary calcium is most commonly achieved through the Agatston score, a semi-quantitative method originally described in 1990.³ To be classified as a calcified lesion, a coronary focus must typically have an attenuation of ≥130 Hounsfield units (HU) and an area of ≥3 contiguous pixels (≈1 mm²) on standard acquisition parameters.³ The Agatston score for a single lesion is calculated by multiplying lesion area by a weighted density factor based on peak attenuation within that lesion: a factor of 1 for 130–199 HU, 2 for 200–299 HU, 3 for 300–399 HU, and 4 for ≥400 HU.³ The total Agatston score is the cumulative sum of scores across the left main, left anterior descending, circumflex, and right coronary arteries.³ While other measures such as calcium volume and mass scores exist, major clinical guidelines and the bulk of outcome evidence continue to prioritize Agatston scoring for routine preventive risk assessment.⁴,⁵
Safety, Cost, and Incidental Findings
Radiation exposure from CAC scanning is generally low, but varies by scanner and protocol. Estimates for CAC screening radiation dose and associated risk have been published, and typical contemporary protocols are often cited around ~1 mSv under optimized conditions.⁶ The field of view includes portions of the lungs, mediastinum, and upper abdomen, so extracardiac incidental findings are not uncommon and may drive downstream testing depending on local reporting practices.³,⁵
Predictive Accuracy and the “Power of Zero” in the General Population
The clinical utility of CAC scoring has been established through large longitudinal cohorts including the Multi-Ethnic Study of Atherosclerosis (MESA), supporting CAC’s ability to refine risk beyond traditional factors.⁷

The Prognostic Impact of a Zero Score
A CAC (Agatston) score of 0 indicates no detectable calcified plaque and is associated with very low short- to intermediate-term event rates in many asymptomatic adults, often supporting downward risk reclassification in appropriate contexts.⁴,⁵,⁷
Why “CAC = 0” can still miss plaque (the key percentages)
CAC detects calcified plaque, not non-calcified plaque. In symptomatic cohorts evaluated with coronary CT angiography (CCTA), clinically meaningful plaque can exist despite CAC=0.
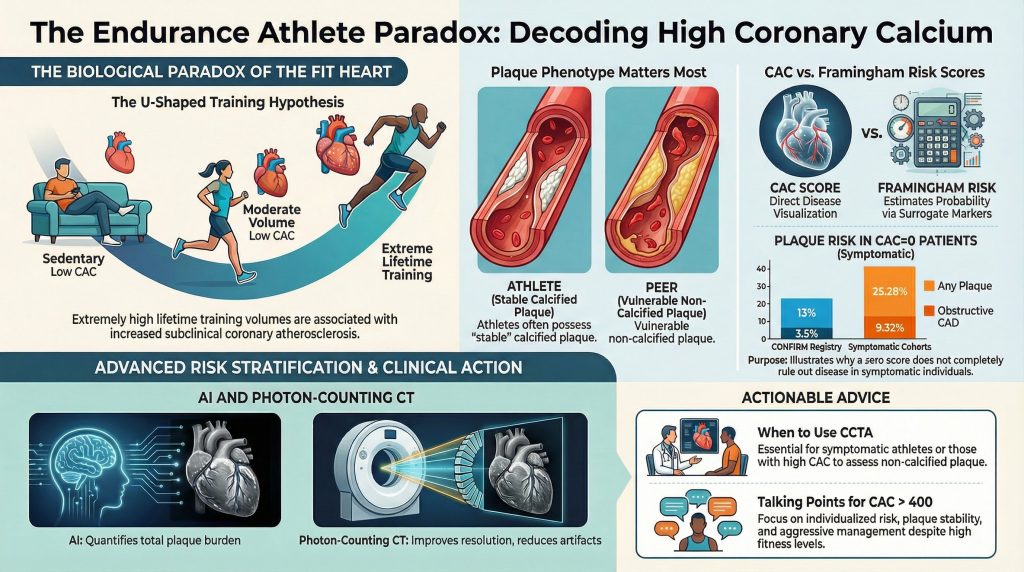
In the CONFIRM registry analysis of symptomatic patients undergoing CCTA, among those with CAC=0, 13% had nonobstructive CAD, 3.5% had ≥50% stenosis, and 1.4% had ≥70% stenosis.⁸
In a large symptomatic cohort study focused on CAC=0 patients undergoing CCTA, 25.28% had any plaque and 9.32% had obstructive CAD.¹⁰
Age materially modifies the “rule-out” value of CAC=0, with younger symptomatic patients more likely to have non-calcified disease.⁹
These findings are the practical reason CAC=0 should not be interpreted as “no coronary disease,” particularly when symptoms are present.
Risk Reclassification and Ethnicity
Traditional risk calculators provide population-based estimates and may misclassify individuals. Adding CAC can improve discrimination and reclassification, especially among patients initially categorized as borderline or intermediate risk.⁴,⁵,⁷
The Paradox of the Endurance Athlete: High CAC in Highly Fit Individuals
The relationship between exercise and heart health is not purely linear. Cardiac imaging studies of masters athletes (often defined as individuals >35 years with years of high-intensity training) have shown that some long-term endurance athletes have higher CAC prevalence and/or greater plaque burden than risk-factor–matched controls.²
Research from the Master@Heart Cohort
In the Master@Heart study, lifelong endurance athletes demonstrated higher coronary atherosclerosis burden compared with controls, emphasizing that increased fitness does not uniformly equate to lower measured plaque burden on imaging.² This has contributed to “U-shaped” or “reverse J-shaped” hypotheses proposing that while moderate exercise is protective, very high lifetime training volumes may be associated with increased subclinical coronary atherosclerosis in some individuals.²

Plaque Phenotype, Fitness, and Event Rates
A key paradox is that despite higher CAC in some endurance athletes, many studies observe favorable outcomes influenced by high cardiorespiratory fitness and overall risk-factor profiles.⁴,¹¹ Still, a high CAC score in an athlete should be interpreted as evidence of underlying atherosclerosis requiring clinical attention and individualized risk discussion—not dismissed as “benign athletic calcification.”²,¹¹
Comparative Analysis: CAC vs. Other Risk Prediction Tools
CAC complements traditional risk scores by providing a direct, disease-based measure. Guidelines support CAC particularly when treatment decisions (e.g., statin initiation) are uncertain in borderline/intermediate-risk patients.⁴,⁵ CCTA directly visualizes both calcified and non-calcified plaque and is therefore better suited to symptomatic evaluation and plaque characterization, but is more complex and typically requires iodinated contrast.³,⁹
Future Directions: Photon-Counting CT and AI-Enabled Plaque Quantification
Photon-counting CT (PCCT) is an emerging CT detector technology that can improve spatial resolution and reduce blooming artifact, potentially improving calcium quantification and plaque characterization in select settings.¹²,¹³
In parallel, AI-enabled quantitative plaque analysis on CCTA has been evaluated in peer-reviewed studies, including REVEALPLAQUE, supporting automated plaque quantification as a step toward more granular anatomic risk assessment beyond a single calcium sum.¹⁴
Conclusion
The coronary artery calcium score is an important tool for cardiovascular risk stratification. By moving beyond statistical probability and visualizing disease burden, CAC enables more individualized primary prevention and shared decision-making.⁴,⁵,⁷ Its “power of zero” can identify individuals at very low near-term risk in the appropriate (asymptomatic) context; however, CAC=0 does not exclude non-calcified plaque, and symptomatic patients can still harbor meaningful plaque and even obstructive disease on CCTA.⁸–¹⁰
In masters endurance athletes, CAC highlights a complex reality: some lifelong athletes demonstrate greater plaque burden and higher CAC, but outcomes are influenced by fitness, risk-factor profiles, and plaque characteristics that vary by cohort.²,¹¹ The practical takeaway remains that CAC is best interpreted in clinical context—useful as a risk modifier and decision aid, not as a stand-alone verdict.⁴,⁵
Corrected References
- Parikh P, Shah N, Ahmed H, Schoenhagen P, Fares M. Coronary artery calcium scoring: Its practicality and clinical utility in primary care. Cleve Clin J Med. 2018;85(9):707-716. doi:10.3949/ccjm.85a.17097
- De Bosscher R, Dausin C, Claus P, et al. Lifelong endurance exercise and its relation with coronary atherosclerosis. Eur Heart J. 2023;44(26):2388-2399. doi:10.1093/eurheartj/ehad152
- Vatsa N, Faaborg-Andersen C, Dong T, Blaha MJ, Shaw LJ, Quintana RA. Coronary Atherosclerotic Plaque Burden Assessment by Computed Tomography and Its Clinical Implications. Circ Cardiovasc Imaging. 2024;17(8):e016443. doi:10.1161/CIRCIMAGING.123.016443
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. doi:10.1161/CIR.0000000000000625
- Foraker R, Sperling L, Bratzke L, et al. Opportunistic Detection of Coronary Artery Calcium on Noncardiac Chest Computed Tomography: An Emerging Tool for Cardiovascular Disease Prevention: A Scientific Statement From the American Heart Association. Circulation. 2025;152(19):e391-e401. doi:10.1161/CIR.0000000000001382
- Kim KP, Einstein AJ, Berrington de González A. Coronary artery calcification screening: estimated radiation dose and cancer risk. Arch Intern Med. 2009;169(13):1188-1194. doi:10.1001/archinternmed.2009.162
- Bild DE, Bluemke DA, Burke GL, et al. Multi-Ethnic Study of Atherosclerosis: objectives and design. Am J Epidemiol. 2002;156(9):871-881. doi:10.1093/aje/kwf113
- Villines TC, Hulten EA, Shaw LJ, et al. Prevalence and severity of coronary artery disease and adverse events among symptomatic patients with coronary artery calcification scores of zero undergoing coronary computed tomography angiography: results from the CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes: An International Multicenter) registry. J Am Coll Cardiol. 2011;58(24):2533-2540. doi:10.1016/j.jacc.2011.10.851
- Mortensen MB, Gaur S, Frimmer A, et al. Association of Age With the Diagnostic Value of Coronary Artery Calcium Score for Ruling Out Coronary Stenosis in Symptomatic Patients. JAMA Cardiol. 2022;7(1):36-44. doi:10.1001/jamacardio.2021.4406
- Yu YT, Hou ZH, Lu B, et al. Prevalence of coronary artery disease in symptomatic patients with zero coronary artery calcium score in different age population. Int J Cardiovasc Imaging. 2021;37(2):723-729. doi:10.1007/s10554-020-02028-8
- DeFina LF, Radford NB, Barlow CE, et al. Association of All-Cause and Cardiovascular Mortality With High Levels of Physical Activity and Concurrent Coronary Artery Calcification. JAMA Cardiol. 2019;4(2):174-181. doi:10.1001/jamacardio.2018.4628
- Symons R, Sandfort V, Mallek M, Ulzheimer S, Pourmorteza A. Coronary artery calcium scoring with photon-counting CT: first in vivo human experience. Int J Cardiovasc Imaging. 2019;35(4):733-739. doi:10.1007/s10554-018-1499-6
- Flohr T, Schmidt B, Ulzheimer S, Alkadhi H. Cardiac imaging with photon counting CT. Br J Radiol. 2023;96(1152):20230407. doi:10.1259/bjr.20230407
- Ramasamy A, Sokooti H, Zhang X, et al. Novel near-infrared spectroscopy-intravascular ultrasound-based deep-learning methodology for accurate coronary computed tomography plaque quantification and characterization. Eur Heart J Open. 2023;3(5):oead090. Published 2023 Oct 30. doi:10.1093/ehjopen/oead090