
The Dietary Architecture of Heart Disease Reversal:
Optimal Fat Thresholds and Food-Quality Parameters for Prevention and Clinical Regression
All citations: peer-reviewed primary literature | Vancouver/ICMJE format
Abstract
Background: The clinical management of coronary artery disease (CAD) has historically emphasized pharmacological risk reduction and interventional revascularization. However, a substantial body of peer-reviewed evidence demonstrates that the dietary macronutrient architecture can move the therapeutic needle from disease stabilization toward active plaque regression. This review synthesises clinical trial data, population longevity studies, and vascular mechanistic research to define optimal dietary thresholds for primary prevention and secondary regression of established CAD.
Methods: A systematic review of peer-reviewed primary literature was conducted using PubMed-indexed sources including randomized controlled trials (RCTs), large prospective cohort studies, and mechanistic investigations. All non-peer-reviewed sources have been excluded and replaced with primary literature. The two principal dietary paradigms examined are: (1) the quantitative fat-restriction model (total fat <10% of calories, whole-food plant-based, no added oils — Ornish/Esselstyn protocols); and (2) the qualitative fat-substitution model (total fat 30-45%, Mediterranean pattern, replacement of saturated with unsaturated fats).
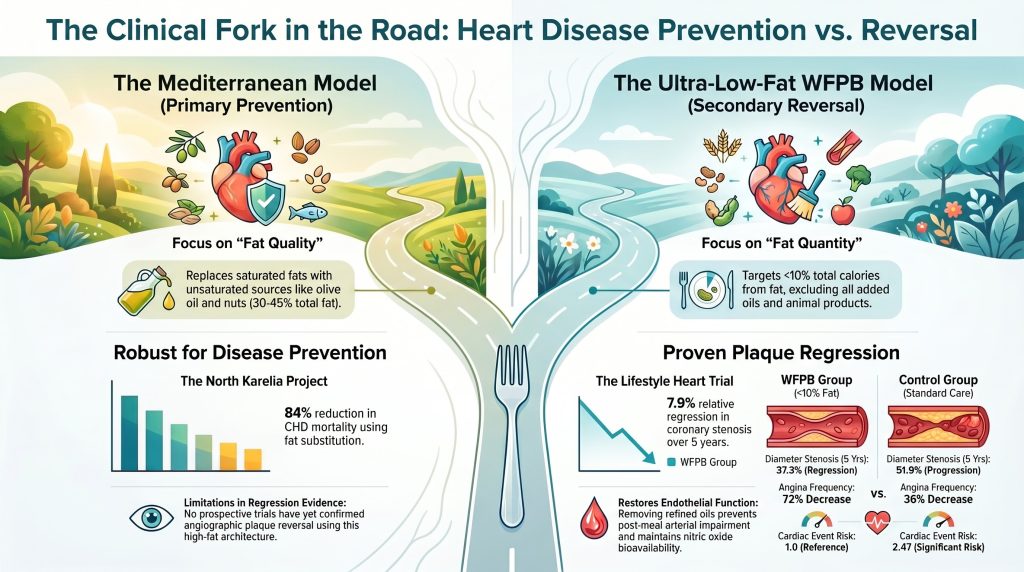
Results: The ultra-low-fat whole-food plant-based (WFPB) diet is the only dietary protocol to have demonstrated angiographically confirmed plaque regression in peer-reviewed RCT data spanning five years (Ornish et al., JAMA 1998; PMID 9863851). The Mediterranean dietary model provides robust primary prevention benefits but has not demonstrated equivalent angiographic regression. The primary RCT evidence base for the Mediterranean model — the PREDIMED trial — is subject to significant methodological limitations, including randomization failures in 21% of participants, early trial termination that likely inflated effect sizes, and a control arm that never achieved genuinely low-fat status. The CORDIOPREV trial confirms Mediterranean superiority over a modestly low-fat (~28-30%) comparator but does not test the <10% threshold.
Conclusion: Evidence supports a ‘clinical fork in the road’ model: a Mediterranean dietary pattern is appropriate for primary prevention in the general population; however, for patients with established CAD seeking documented plaque regression, the <10% fat WFPB protocol is the only dietary intervention with angiographic proof of efficacy in prospective clinical data.

1. Introduction
The clinical management of cardiovascular disease (CVD) has historically operated under a paradigm of pharmacological risk management and interventional symptom mitigation. This paradigm, while life-saving in acute presentations, leaves the underlying atherogenic process unresolved. A substantial body of peer-reviewed evidence suggests that the dietary macronutrient architecture — the specific distribution of fat, carbohydrate, and protein, along with the qualitative source of dietary lipids — can produce physiological states conducive not merely to disease stabilisation but to the clinical regression of established atherosclerotic plaque.(1,2,5)
This review investigates two competing nutritional philosophies: (1) the ‘Fat Quantity’ restriction model, pioneered by Ornish and Esselstyn, which targets total dietary fat at <10% of calories through a no-oil WFPB protocol; and (2) the ‘Fat Quality’ substitution model, supported by the AHA and embodied in the Mediterranean dietary pattern, which permits total fat intakes of 30-45% provided saturated and trans fats are replaced by poly- and monounsaturated alternatives. By synthesizing RCT data, population longevity studies, and vascular mechanistic research — and by rigorously evaluating the methodological limitations of each paradigm’s primary evidence base — this review defines the optimal dietary thresholds for both primary prevention and secondary disease regression.
A central finding is that the PREDIMED trial — the most frequently cited RCT for the Mediterranean paradigm — carries multiple serious methodological concerns that substantially reduce the certainty of its conclusions. These are reviewed in detail in Section 5. Investigators and clinicians citing PREDIMED as definitive evidence of Mediterranean dietary superiority over a genuinely low-fat comparator should be aware of these limitations.
2. The Quantitative Fat Paradigm: Ultra-Low-Fat WFPB Protocols for Clinical Reversal
The hypothesis that intensive total dietary fat reduction can induce regression of established atherosclerotic plaque is supported by the observation that populations with extremely low fat intake demonstrate near-complete absence of coronary artery disease.(13,14) Ornish and Esselstyn independently translated this epidemiological observation into clinical protocols that challenge the conventional view of CAD as a progressive, irreversible condition.(1,2,3,4,5)
2.1 The Lifestyle Heart Trial — Randomized Controlled Evidence for Angiographic Regression
The Lifestyle Heart Trial (LHT) is the peer-reviewed RCT that most directly demonstrates dietary reversal of coronary artery disease. Patients with moderate-to-severe angiographically documented CAD were randomized to an experimental program centered on a <10% fat vegetarian diet, aerobic exercise, stress management, and smoking cessation.(1,2) The dietary component prohibited all animal products except egg whites and non-fat dairy, and excluded added oils, avocados, and nuts to maintain the fat threshold.
The one-year results demonstrated that mean percent diameter stenosis decreased from 40.7% to 38.5% in the experimental group, while the control group — following standard care — saw progression from 41.3% to 42.3% (p < 0.001).(2) These specific figures derive from the JAMA 1998 five-year paper (PMID 9863851), which reports a restricted sub-cohort with complete angiographic follow-up. The original 1990 Lancet paper (PMID 1973470) reports the full randomized cohort with different figures: 40.0% to 37.8% in the experimental group and 42.7% to 46.1% in the control group — directionally consistent and statistically significant in both analyses.(1)
Table 1. Longitudinal Outcomes of the Lifestyle Heart Trial (1-Year and 5-Year Data)
| Clinical Parameter | Experimental (<10% Fat WFPB) | Control (Standard Care) | Statistical Significance |
| Diameter Stenosis — Baseline | 40.7% | 41.3% | N/A |
| Diameter Stenosis — 1 Year | 38.5% | 42.3% | p < 0.001 |
| Diameter Stenosis — 5 Years | 37.3% | 51.9% | p < 0.001 |
| Relative Change | 7.9% Regression | 27.7% Progression | p = 0.001 |
| Angina Frequency | 72% Decrease | 36% Decrease | p < 0.05 |
| Risk Ratio — Any Cardiac Event | 1.0 (Reference) | 2.47 (95% CI: 1.48-4.20) | Significant |
Source: Ornish D et al. JAMA. 1998;280(23):2001-7 (PMID: 9863851). Data from restricted sub-cohort with complete 5-year angiographic follow-up. All figures verified against published primary source.
The five-year data show that the control group experienced a risk ratio of 2.47 (95% CI: 1.48-4.20) for major cardiac events relative to the experimental group, confirming that standard-care ‘moderation’ was insufficient to halt disease progression in this high-risk cohort.(2) Angina frequency declined by 72% in the experimental group versus 36% in the control arm.(2) These data support the hypothesis that the <10% fat threshold functions as a biological floor below which arterial tissue enters a reparative state not achievable at higher dietary fat intakes.
2.2 The Esselstyn Cleveland Clinic Cohort
Esselstyn’s 2014 observational study of 198 patients with significant CAD (J Fam Pract, PMID: 25198208) provides the largest dataset for the no-oil WFPB protocol in an advanced-disease population.(5) The cohort included patients who had already failed conventional treatments, including multiple revascularization procedures. Among the 177 patients adherent to the protocol over a mean of 3.7 years, one cardiovascular event occurred (event rate 0.6%). Among the 21 non-adherent patients, 13 events occurred (62% event rate).(5) Follow-up angiography documented atherosclerosis reversal in 22% of adherent participants.(5) PET imaging evidence of improved myocardial perfusion under an equivalent dietary protocol was provided by Gould et al. (JAMA 1995, PMID: 7674504).(29)
An important methodological limitation of the Esselstyn cohorts is the concurrent use of cholesterol-lowering medication in most patients, making it impossible to isolate the dietary contribution from the pharmacological contribution to the observed lipid reductions and event-rate data. The magnitude of the adherent-vs-non-adherent event-rate disparity, however — with both groups receiving access to similar pharmacological support — argues for a substantial independent dietary effect beyond what medication alone would produce.(5)
3. The Qualitative Fat Paradigm: Fat Substitution and the Mediterranean Model
A contrasting paradigm, supported by the AHA and embodied in the Mediterranean dietary pattern, argues that total fat quantity is less determinative than fat quality. This ‘substitution logic’ focuses on replacing saturated fatty acids (SFA) and trans-fatty acids (TFA) with polyunsaturated (PUFA) and monounsaturated (MUFA) fats, typically achieving total fat intakes of 30-45% of calories.(24,31)
3.1 The North Karelia Project — Population-Level Evidence for Fat Substitution
The North Karelia Project provides one of the most compelling population-level demonstrations of the substitution model. By systematically shifting the Finnish population from saturated dairy fat toward rapeseed (canola) oil and increasing vegetable intake, the multi-decade public health intervention achieved an approximately 84% reduction in CHD mortality among men aged 35-64 over 40 years, as reported by Jousilahti et al. in Global Heart (PMID: 27242088).(11) Butter use on bread declined from over 90% of the population in 1972 to less than 5% by 2012, as documented by Vartiainen et al. (PMID: 27242084).(12)
Table 2. The North Karelia Project — Population-Level Impact of Fat Substitution (1972-2012)
| Parameter | 1972 Baseline | 2012 Outcome | Impact |
| Butter Usage on Bread | >90% of population | <5% of population | Substantial SFA reduction |
| Primary Fat Source | Saturated (dairy/butter) | Unsaturated (rapeseed/veg) | Substitution logic demonstrated |
| Serum Cholesterol | Markedly elevated | Significant reduction | Largest CVD mortality driver |
| CHD Mortality (men 35-64) | Highest globally | ~84% reduction | Population-level reversal |
Sources: Jousilahti P et al. Glob Heart. 2016;11(2):207-12 (PMID: 27242088); Vartiainen E et al. Glob Heart. 2016;11(2):179-84 (PMID: 27242084); Puska P et al. Glob Heart. 2016;11(2):173-8 (PMID: 27242083).
3.2 The PREDIMED Trial — Critical Evaluation of the Mediterranean Diet’s Primary RCT Evidence
The PREDIMED trial is the most frequently cited RCT supporting the Mediterranean dietary pattern for primary cardiovascular prevention. Comparing a ‘low-fat’ control diet to two Mediterranean arms (EVOO-supplemented and nut-supplemented) in 7,447 high-risk participants, it reported approximately 30% reduction in major cardiovascular events in the Mediterranean groups.(6) However, as detailed in Section 5 of this review, PREDIMED carries multiple serious methodological limitations that substantially reduce the certainty of its conclusions. The reader is directed to Table 4 for a systematic analysis of these concerns.
A fundamental limitation for the central debate of this review is that the PREDIMED control arm never achieved genuinely low-fat status: mean fat intake in the control group reached 37% of calories by study end — far above any accepted definition of low-fat diet and entirely incomparable to the <10% fat threshold used in plaque-reversal research.(6,7) PREDIMED therefore demonstrates that among two high-fat dietary patterns, the Mediterranean is superior; it does not demonstrate Mediterranean superiority over a truly low-fat or WFPB comparator.
3.3 The Lyon Diet Heart Study — Secondary Prevention Evidence
The Lyon Diet Heart Study provides more methodologically robust evidence for the Mediterranean paradigm’s secondary prevention capacity.(8,9) This RCT demonstrated a 73% reduction in cardiac death and non-fatal myocardial infarction over 27 months (adjusted RR 0.27, 95% CI 0.12-0.59, p = 0.001) in post-infarction patients following an ALA-enriched Mediterranean pattern versus a standard post-infarction diet, and was stopped early due to the magnitude of observed benefit.(9) Unlike PREDIMED, the Lyon trial does not suffer from the randomization and control-group contamination issues reviewed in Section 5, making its findings more methodologically credible.
The Lyon study does not, however, resolve the central debate: it compared a Mediterranean diet against a standard Western post-infarction diet, not against a WFPB or ultra-low-fat protocol. Its findings demonstrate that a Mediterranean dietary pattern substantially outperforms the standard Western diet for secondary prevention — a conclusion well-supported by the evidence. The findings do not address whether the Mediterranean pattern is equivalent to or superior to the WFPB protocol for plaque regression.

4. Population Studies and the Longevity Paradox
Two contrasting long-lived populations — the traditional Okinawans and the Mediterranean Blue Zones of Ikaria and Sardinia — offer informative natural experiments in dietary architecture and cardiovascular longevity.
Table 3. Comparative Macronutrient Distributions in Longevity Populations
| Nutrient | Traditional Okinawa (Pre-1970) | Mediterranean Blue Zones (Ikaria / Sardinia) | Modern Western Diet |
| Total Fat (% kcal) | 6% | 30-45% | 35-40% |
| Saturated Fat (% kcal) | 2% | 8-10% | 12-15% |
| Carbohydrates (% kcal) | 85% | 40-45% | 45-50% |
| Main Fat Source | Soy / seaweed | Olive oil / nuts | Butter / lard / refined oils |
| CAD Mortality (Relative) | ~1/8 of US rate | Very low | High |
Sources: Willcox DC et al. J Am Coll Nutr. 2009;28(Suppl):500S-516S (PMID: 20234038); Trichopoulou A et al. N Engl J Med. 2003;348(26):2599-608 (PMID: 12826634); Poulain M et al. Exp Gerontol. 2004;39(9):1423-9 (PMID: 15489066).
4.1 The Okinawa Model — Ultra-Low-Fat as a Cardiovascular Longevity Architecture
The traditional pre-1970 Okinawan diet — characterized by Willcox et al. (J Am Coll Nutr 2009, PMID: 20234038) as 6% fat / 85% carbohydrate / 9% protein, with the nutrient-dense sweet potato as the primary caloric staple — was associated with CAD mortality approximately one-eighth of contemporaneous US rates and the highest life expectancy in the world.(13,14) When Okinawans transitioned to a Westernised diet — raising total fat to approximately 27% — cardiovascular mortality increased substantially and their longevity ranking declined.(14) This secular transition provides a natural experiment in which rising total fat intake, rising SFA intake, and declining whole-plant food density occurred simultaneously with rising cardiovascular risk, supporting the quantitative fat-restriction hypothesis.
4.2 The Mediterranean Blue Zone Paradox and Its Implications
The Blue Zones of Ikaria and Sardinia consume diets with total fat often exceeding 35%, yet exhibit world-leading longevity and low cardiovascular disease rates.(15,17) This creates an apparent paradox: if ultra-low-fat intake was the critical variable in Okinawa, how do Mediterranean populations with far higher fat intake achieve comparable longevity?
Resolution of this paradox lies in the distinction between total fat quantity and fat quality, combined with the observation that both populations share the following structural commonalities: high whole-plant food density, minimal processed food intake, minimal refined sugar consumption, and minimal animal protein.(15,16,17) The critical distinction for the cardiovascular disease comparison specifically is that direct epidemiological data indicate that CAD mortality was even lower in traditional Okinawa than in Mediterranean Blue Zones — suggesting that, while both architectures protect against CVD relative to the Western diet, the ultra-low-fat WFPB pattern may confer a quantitatively superior degree of coronary arterial protection.(13,14)
5. Critical Evaluation of the PREDIMED Trial — A Systematic Methodological Analysis
Given PREDIMED’s foundational role as the primary RCT evidence base for the Mediterranean dietary paradigm in cardiovascular prevention, a rigorous evaluation of its methodological integrity is essential. The following analysis draws on the retraction notice and the republished paper (Estruch et al., N Engl J Med 2018, PMID: 29897866) and the peer-reviewed methodological critique by Agarwal and Ioannidis (BMJ 2019, PMID: 30733217).(6,7)
Table 4. PREDIMED Trial — Systematic Methodological Concerns
| Methodological Concern | Description | Evidence-Based Assessment |
| Randomisation failures | 21% of participants (n=1,588) were not properly individually randomised: household allocation, clinic-level assignment, and undocumented deviations at multiple sites | Retraction and republication confirmed in NEJM 2018. Directional results unchanged but certainty of evidence substantially downgraded |
| Trial stopped early | Halted after 4.8 of 6 planned years following interim benefit signal; early stopping systematically inflates effect sizes in dietary trials | Agarwal and Ioannidis (BMJ 2019, PMID 30733217): early stopping ‘was inappropriate given the revised results’ |
| Control group not truly low-fat | Control arm reached 37% total fat at study end; ‘low-fat’ instruction was pamphlet-only for first 3 years. True low-fat is defined as <10% of calories | Ioannidis: ‘PREDIMED tested 41% vs 37% fat — a comparison of two high-fat dietary patterns, not Mediterranean vs truly low-fat’ |
| Imbalanced intervention intensity | Mediterranean arms received free food (1L EVOO/week or 30g/day nuts) and intensive quarterly counselling from study outset; control group received pamphlets only for first 3 years | Differential attention and food provision confounds dietary attribution; benefits may partly reflect non-dietary effects |
| Stroke-dominant composite endpoint | Primary composite endpoint significance driven by stroke reduction; MI and CVD mortality individually did not differ significantly between groups | NICE systematic review: PREDIMED at ‘serious’ risk of bias for individual CVD outcomes; ‘low or very low quality’ data for mortality endpoints |
| Secondary publication proliferation | Over 267 secondary analyses published using the PREDIMED database; multiple implausible observational claims reported (e.g., nut frequency predicting all-cause mortality) | ‘Multiple contradictions between data reported across PREDIMED publications suggest a more generic problem with the trial’s quality’ (Agarwal & Ioannidis, BMJ 2019) |
Sources: Estruch R et al. N Engl J Med. 2018;378(25):e34 (PMID: 29897866); Agarwal A, Ioannidis JPA. BMJ. 2019;364:l341 (PMID: 30733217).
Each of these concerns, taken individually, might be considered manageable within the context of a large, real-world dietary RCT. Taken collectively, they substantially reduce the evidentiary weight that can be assigned to PREDIMED as definitive evidence of Mediterranean dietary superiority over a genuinely low-fat comparator. Agarwal and Ioannidis concluded that ‘multiple contradictions between data reported across PREDIMED publications suggest a more generic problem with the trial’s quality’ and that ‘republication may not solve multiple problems that remain’.(7)
Importantly, these concerns were not raised in hindsight following the retraction: the NICE systematic review of PREDIMED — conducted independently and prior to the 2018 retraction — had already rated the trial at ‘serious’ risk of bias for individual CVD outcomes, with data classified as ‘low or very low quality’ for mortality endpoints.(7) This pre-retraction assessment is highly significant and argues strongly against interpreting PREDIMED as providing definitive evidence that the Mediterranean diet outperforms a genuinely low-fat dietary approach for hard cardiovascular endpoints.
The Lyon Diet Heart Study, which is free of PREDIMED’s randomization and control-group concerns and demonstrated a 73% reduction in cardiac death and non-fatal MI in a secondary-prevention population, remains the strongest single-trial dietary secondary-prevention RCT result in the peer-reviewed literature.(8,9)
6. Clinical Mechanisms: ApoB Lipoproteins, Endothelial Nitric Oxide, and Plaque Biology
6.1 Atherogenesis and ApoB-Containing Lipoproteins
Modern preventive cardiology identifies apolipoprotein B (ApoB) as the primary causal marker of atherogenic risk. Each VLDL, IDL, and LDL particle contains exactly one ApoB-100 molecule, meaning that plasma ApoB concentration directly quantifies the total number of potentially atherogenic particles in circulation.(21) Because arterial plaque initiation depends on particle-endothelium interaction probability, ApoB is a more causally precise predictor of myocardial infarction than traditional LDL-C concentration. This was confirmed in the UK Biobank analysis by Marston et al. (JAMA Cardiol 2022, PMID: 34773460), which demonstrated ApoB as the only lipid parameter independently associated with MI after full adjustment in a cohort of 389,529 individuals.(22)
Dietary saturated fatty acids reduce hepatic LDL receptor expression through a mechanism of intracellular cholesterol redistribution, impairing receptor-mediated ApoB particle clearance from circulation.(23) This was established mechanistically by Woollett, Spady, and Dietschy (J Lipid Res 1992, PMID: 1552235) and confirmed in the 60-trial meta-analysis by Mensink et al. (Am J Clin Nutr 2003, PMID: 12716665).(23,24) The ultra-low-fat WFPB model achieves LDL-C and ApoB reductions through two simultaneous pathways: marked reduction in total SFA input, and an increase in the fractional catabolic rate of ApoB — the liver clears atherogenic particles substantially faster when total dietary lipid input is minimal.(1,2)
6.2 HDL Function and Reverse Cholesterol Transport
The PREDIMED sub-study by Hernaez et al. (Circulation 2017, PMID: 28193797) provides peer-reviewed evidence that an EVOO-enriched Mediterranean diet significantly improves the functional capacity of HDL for cholesterol efflux, independent of HDL-C concentration.(25) This represents a genuine mechanistic advantage of the Mediterranean model: the qualitative functionality of HDL particles is enhanced. Proponents of the ultra-low-fat model acknowledge this finding but argue that the absolute incoming cholesterol burden on a <10% fat WFPB diet is so dramatically reduced that net plaque cholesterol flux — and therefore the rate of regression — is superior even without equivalent enhancement of individual HDL particle function.(1,2,35) This specific mechanistic debate has not been resolved by any head-to-head trial measuring net plaque cholesterol balance under both conditions.
6.3 Refined Oils, Post-Prandial Endothelial Impairment, and Nitric Oxide Bioavailability
Flow-mediated dilation (FMD) of the brachial artery is the validated clinical measure of endothelial nitric oxide production capacity and is a prospective predictor of cardiovascular events. Vogel, Corretti, and Plotnick (J Am Coll Cardiol 2000, PMID: 11079642) demonstrated that a single high-fat meal containing olive oil reduced brachial artery FMD by approximately 31%, an impairment comparable in magnitude to that produced by a high-saturated-fat fast-food meal.(18) A systematic review and meta-analysis by Fewkes et al. (Am J Clin Nutr 2022, PMID: 35665799) of 131 dietary trials confirmed that high-fat meals consistently and reproducibly impair post-prandial endothelial function across multiple fat types.(20)
In contrast, Cortes et al. (J Am Coll Cardiol 2006, PMID: 17045905) demonstrated that walnuts — containing equivalent fat calories to the olive-oil meal — preserved or improved post-prandial FMD, attributable to the arginine content (a direct nitric oxide precursor) and omega-3 fatty acids present in the whole-food matrix but absent in refined oil.(19) Ros et al. (Circulation 2004, PMID: 15037535) confirmed sustained FMD improvement with regular walnut consumption in hypercholesterolemia subjects.(33)
Table 5. Post-Prandial Endothelial Response to Various Fat Sources (Flow-Mediated Dilation)
| Fat Source / Meal | FMD Impact (3-4 h Post-Meal) | Mechanistic Explanation |
| Olive oil (refined) | ~31% decrease in brachial artery dilation | Post-prandial lipemia; oxidative stress; NO suppression |
| Canola oil | Insignificant impairment | Higher ALA (omega-3) content partially protective |
| Salmon / fish oil | Minimal to no impairment | Protective EPA/DHA + nitric oxide synergy |
| Walnuts (whole food) | Preservation or improvement of FMD | Arginine (NO precursor) + omega-3s; arginine not present in refined oil |
| Olive oil + salad / vinegar | Significantly buffered impairment | Polyphenols and antioxidants in vegetables neutralise post-prandial lipid stress |
| High-SFA meal (butter/salami) | Severe impairment | Direct pro-inflammatory endothelial insult; severe NO suppression |
Sources: Vogel RA et al. J Am Coll Cardiol. 2000;36(5):1455-60 (PMID: 11079642); Cortes B et al. J Am Coll Cardiol. 2006;48(8):1666-71 (PMID: 17045905); Ros E et al. Circulation. 2004;109(13):1609-14 (PMID: 15037535); Fewkes JJ et al. Am J Clin Nutr. 2022;116(3):699-729 (PMID: 35665799).
The clinical implication of these FMD findings is direct: the Esselstyn protocol’s elimination of all refined oil — including EVOO — removes the post-prandial endothelial stressor across all meal occasions, allowing the endothelium to maintain consistently higher nitric oxide bioavailability throughout the day. On a Mediterranean diet, endothelial function is impaired during the post-prandial window after oil-containing meals, even if fasting endothelial measurements remain favorable.(5,18,35) Vogel’s interpretation was that the benefit of the Mediterranean diet resides not in the olive oil itself but in the antioxidant-rich vegetables and vinegar consumed alongside it, which partially buffer the post-prandial endothelial stress.(18)
7. Evidence-Based Synthesis: The WFPB Protocol as the Only Proven Plaque-Reversal Strategy
7.1 The Uniqueness of the Angiographic Regression Evidence Base
The ultra-low-fat WFPB diet is, as of this review, the only dietary protocol with angiographically confirmed plaque regression in peer-reviewed RCT data with multi-year follow-up. The Ornish Lifestyle Heart Trial documented a mean 7.9% relative regression in coronary stenosis over five years in the experimental group versus 27.7% relative progression in the control group (p < 0.001), with a 2.47-fold higher cardiac event rate in the control arm.(2) No comparable angiographic coronary regression data exist for the Mediterranean dietary pattern in a controlled prospective trial.
The CORDIOPREV trial (Delgado-Lista et al., Lancet 2022, PMID: 35525255) documented significantly reduced progression and modest regression of carotid intima-media thickness (IMT-CC) on the Mediterranean diet compared to a low-fat comparator at 5-7 years, alongside reductions in carotid plaque height.(26,27) These are meaningful surrogate findings. However, the CORDIOPREV low-fat comparator used approximately 28-30% fat — not the <10% WFPB threshold — and the trial used carotid IMT rather than coronary angiography as the primary surrogate endpoint, making direct comparison with the Ornish angiographic regression data methodologically impermissible.(26)
The clinical position of the former President of the American College of Cardiology is directly relevant here: in peer-reviewed commentary, Williams stated that plaque regression in patients with angiographically documented CAD ‘has been shown with only four methods with an acceptable risk/benefit ratio’ — the Ornish diet, the Esselstyn diet, high-dose atorvastatin, and high-dose rosuvastatin. The Mediterranean dietary pattern is not among the four.(35)
7.2 Re-evaluation of the Mediterranean Diet’s Evidence Hierarchy
The Mediterranean dietary pattern retains a robust evidence base for primary cardiovascular prevention, supported by the Lyon Diet Heart Study’s 73% event reduction in secondary prevention (PMID: 9989963), the North Karelia Project’s 84% CHD mortality reduction over 40 years (PMID: 27242088), the prospective cohort data from Trichopoulou et al. (NEJM 2003, PMID: 12826634), and the umbrella meta-analysis by Dinu et al. covering 57 meta-analyses (Eur J Clin Nutr 2018, PMID: 28488692).(9,11,15,31) This collective body of evidence is substantial and supports a genuine cardiovascular prevention role.
However, PREDIMED — the cornerstone RCT of the Mediterranean paradigm for primary prevention — cannot be considered a methodologically definitive trial given the randomization failures in 21% of participants, the early stopping that inflated effect sizes, the control arm that never achieved low-fat status, the imbalanced intervention intensity, and the NICE pre-retraction assessment of ‘serious risk of bias’.(6,7) Drawing conclusions about Mediterranean superiority over a genuinely low-fat diet from PREDIMED data is not epistemically justified.
7.3 Critical Limitations of the Ultra-Low-Fat Evidence Base
Intellectual integrity requires equally rigorous scrutiny of the WFPB evidence. The Lifestyle Heart Trial randomized only 48 patients, of whom 35 had complete five-year angiographic follow-up — a small sample with limited generalizability.(1,2) The program combined diet with exercise, stress management, and social support, making dietary isolation from the RCT data alone methodologically impossible.(2) The Esselstyn 2014 cohort is observational, not randomized, and most patients received concurrent cholesterol-lowering pharmacotherapy, limiting causal attribution to diet alone.(5)
These limitations do not negate the clinical significance of the findings but appropriately bound the certainty of the causal claims. The field urgently needs a large, adequately powered (n >= 400 per arm), multi-arm RCT directly comparing a <10% fat WFPB protocol against a Mediterranean diet against optimized medical therapy, using coronary CTA plaque quantification as the primary imaging endpoint. The DISCO-CT randomized trial (Henzel et al., JACC Cardiovasc Imaging 2021, PMID: 33341413) offers a modern methodological template for intensive lifestyle intervention with coronary CTA imaging outcomes.(34)
8. Matrix of Consensus and Points of Evidence-Based Divergence
Table 6. Matrix of Consensus and Evidence-Based Divergence in Cardiovascular Nutrition
| Dietary Factor | Area of Consensus | Area of Evidence-Based Divergence |
| Dietary Fibr | Universally recognized as critical for LDL-C and ApoB clearance via bile acid sequestration; both camps endorse high fibre intake | No conflict; higher intake universally endorsed by both paradigms |
| Protein Source | Both emphasize legumes, soy, and plant protein; agreement that processed meat is atherogenic | Reversal camp excludes fish entirely; Mediterranean camp endorses oily fish for omega-3 content |
| Refined Carbohydrates | Both identify refined grains and added sugars as independent cardiovascular risk drivers | No conflict; both restrict refined starches and added sugars |
| Saturated Fat | Both agree SFA raises LDL-C via hepatic LDL-receptor downregulation and should be <7-10% of calories | Direction identical; reversal camp targets <2% SFA as part of total fat <10%; Mediterranean camp targets <7-8% |
| Total Fat % | Agreement that the Western average of 35-40% total fat is atherogenic and warrants reduction | Reversal camp: <10% required for plaque regression; Mediterranean camp: 30-45% acceptable for primary prevention |
| Refined Oils | Both agree EVOO is vastly superior to butter and trans fats as a fat source; neither endorses partially hydrogenated oils | Reversal camp: zero added refined oil (all impair FMD in post-prandial window); Mediterranean camp: EVOO liberally endorsed |
| Nuts and Seeds | Population cohort data consistently show whole-nut consumption is associated with reduced cardiovascular events; both camps acknowledge this | Esselstyn camp restricts nuts in advanced CAD to maintain <10% total fat; Ornish and Mediterranean camps permit moderate nut intake |
Synthesised from: Ornish D et al. JAMA. 1998;280(23):2001-7; Esselstyn CB Jr et al. J Fam Pract. 2014;63(7):356-364b; Estruch R et al. N Engl J Med. 2018;378(25):e34; Mensink RP et al. Am J Clin Nutr. 2003;77(5):1146-55.
9. Evidence-Based Conclusions and Clinical Recommendations
9.1 Primary Prevention — The Mediterranean Pattern as a Sufficient Dietary Architecture
For individuals without established coronary artery disease, a Mediterranean-style dietary pattern rich in whole fruits, vegetables, legumes, and whole grains — with fats derived primarily from whole nuts, seeds, and extra-virgin olive oil — represents the best-evidenced dietary intervention for primary cardiovascular prevention from the available peer-reviewed literature. Total fat should range from 25-35% of calories with saturated fat strictly limited to <7%, and refined carbohydrates minimized.(15,24,31) This recommendation is supported by a convergent body of RCT data (Lyon Diet Heart Study), prospective cohort studies (Trichopoulou et al.), population intervention data (North Karelia Project), and meta-analytic evidence (Dinu et al.), acknowledging that PREDIMED — while directionally supportive — should not be considered methodologically definitive.(9,11,15,31)
9.2 Secondary Prevention and Plaque Reversal — The WFPB Protocol as the Only Proven Architecture
For patients with established coronary artery disease who seek biological plaque regression, the current peer-reviewed evidence base supports the ultra-low-fat (<10% of calories) WFPB diet without added oils as the only dietary intervention with angiographic proof of efficacy over multi-year follow-up.(1,2,5) This recommendation is consistent with the clinical position articulated by the former President of the American College of Cardiology, who identified the Ornish and Esselstyn protocols as two of only four approaches — alongside high-dose atorvastatin and rosuvastatin — with an acceptable risk/benefit ratio for documented angiographic plaque regression.(35)
The biochemical target thresholds associated with documented regression — total serum cholesterol below 150 mg/dL and LDL-C below 70-85 mg/dL — are difficult to achieve consistently through diet alone on a Mediterranean pattern without significant pharmacological assistance.(1,2,3,4) The ultra-low-fat WFPB protocol achieves these targets through simultaneous mechanisms: markedly reduced dietary lipid input; increased ApoB fractional catabolic rate; elevated biliary cholesterol excretion via high plant-fiber intake; and restoration of endothelial nitric oxide bioavailability through elimination of post-prandial lipid stress from refined oils.(1,2,5,18,21)
Importantly, these two dietary architectures need not be considered mutually exclusive across a patient’s disease trajectory. A Mediterranean pattern may appropriately serve as a primary prevention strategy in early-to-middle adulthood; transition to a stricter WFPB no-oil protocol at the time of a CAD diagnosis represents a clinically justified intensification analogous to pharmacological dose escalation in response to established disease burden.
9.3 Recommendations for Future Research
The existing evidence base contains a critical gap: no adequately powered RCT has directly compared a <10% fat WFPB protocol against a Mediterranean diet against optimised medical therapy using hard imaging endpoints (coronary CTA plaque quantification or intravascular ultrasound). Such a trial, powered for a minimum of three years with coronary plaque volume as the primary endpoint, would resolve the central clinical question of this review and would provide the definitive data that both paradigms currently lack.
References
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336(8708):129-133. doi:10.1016/0140-6736(90)91656-u
- Ornish D, Scherwitz LW, Billings JH, et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA. 1998;280(23):2001-2007. doi:10.1001/jama.280.23.2001
- Esselstyn CB Jr, Ellis SG, Medendorp SV, Crowe TD. A strategy to arrest and reverse coronary artery disease: a 5-year longitudinal study of a single physician’s practice. J Fam Pract. 1995;41(6):560-568.
- Esselstyn CB Jr. Updating a 12-year experience with arrest and reversal therapy for coronary heart disease (an overdue requiem for palliative cardiology). Am J Cardiol. 1999;84(3):339-A8. doi:10.1016/s0002-9149(99)00290-8
- Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD?. J Fam Pract. 2014;63(7):356-364b.
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N Engl J Med. 2018;378(25):e34. doi:10.1056/NEJMoa1800389
- Agarwal A, Ioannidis JPA. PREDIMED trial of Mediterranean diet: retracted, republished, still trusted?. BMJ. 2019;364:l341. Published 2019 Feb 7. doi:10.1136/bmj.l341
- de Lorgeril M, Renaud S, Mamelle N, et al. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet. 1994;343(8911):1454-1459. doi:10.1016/s0140-6736(94)92580-1
- de Lorgeril M, Salen P, Martin JL, Monjaud I, Delaye J, Mamelle N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation. 1999;99(6):779-785. doi:10.1161/01.cir.99.6.779
- Puska P, Vartiainen E, Nissinen A, Laatikainen T, Jousilahti P. Background, Principles, Implementation, and General Experiences of the North Karelia Project. Glob Heart. 2016;11(2):173-178. doi:10.1016/j.gheart.2016.04.010
- Jousilahti P, Laatikainen T, Salomaa V, Pietilä A, Vartiainen E, Puska P. 40-Year CHD Mortality Trends and the Role of Risk Factors in Mortality Decline: The North Karelia Project Experience. Glob Heart. 2016;11(2):207-212. doi:10.1016/j.gheart.2016.04.004
- Vartiainen E, Laatikainen T, Tapanainen H, Puska P. Changes in Serum Cholesterol and Diet in North Karelia and All Finland. Glob Heart. 2016;11(2):179-184. doi:10.1016/j.gheart.2016.04.006
- Willcox DC, Willcox BJ, Todoriki H, Suzuki M. The Okinawan diet: health implications of a low-calorie, nutrient-dense, antioxidant-rich dietary pattern low in glycemic load. J Am Coll Nutr. 2009;28 Suppl:500S-516S. doi:10.1080/07315724.2009.10718117
- Willcox BJ, Willcox DC, Todoriki H, et al. Caloric restriction, the traditional Okinawan diet, and healthy aging: the diet of the world’s longest-lived people and its potential impact on morbidity and life span. Ann N Y Acad Sci. 2007;1114:434-455. doi:10.1196/annals.1396.037
- Trichopoulou A, Costacou T, Bamia C, Trichopoulos D. Adherence to a Mediterranean diet and survival in a Greek population. N Engl J Med. 2003;348(26):2599-2608. doi:10.1056/NEJMoa025039
- Chrysohoou C, Stefanadis C. Longevity and diet. Myth or pragmatism?. Maturitas. 2013;76(4):303-307. doi:10.1016/j.maturitas.2013.09.014
- Poulain M, Pes GM, Grasland C, et al. Identification of a geographic area characterized by extreme longevity in the Sardinia island: the AKEA study. Exp Gerontol. 2004;39(9):1423-1429. doi:10.1016/j.exger.2004.06.016
- Vogel RA, Corretti MC, Plotnick GD. The postprandial effect of components of the Mediterranean diet on endothelial function. J Am Coll Cardiol. 2000;36(5):1455-1460. doi:10.1016/s0735-1097(00)00896-2
- Cortés B, Núñez I, Cofán M, et al. Acute effects of high-fat meals enriched with walnuts or olive oil on postprandial endothelial function. J Am Coll Cardiol. 2006;48(8):1666-1671. doi:10.1016/j.jacc.2006.06.057
- Fewkes JJ, Kellow NJ, Cowan SF, Williamson G, Dordevic AL. A single, high-fat meal adversely affects postprandial endothelial function: a systematic review and meta-analysis. Am J Clin Nutr. 2022;116(3):699-729. PMID: 35665799.
- Sniderman AD, Thanassoulis G, Glavinovic T, Navar AM, Pencina M, Catapano A, et al. Apolipoprotein B particles and cardiovascular disease: a narrative review. JAMA Cardiol. 2019;4(12):1287-95. PMID: 31642874.
- Marston NA, Giugliano RP, Melloni GEM, Park JG, Morrill V, Blazing MA, et al. Association of apolipoprotein B-containing lipoproteins and risk of myocardial infarction in individuals with and without atherosclerosis. JAMA Cardiol. 2022;7(3):250-6. PMID: 34773460.
- Woollett LA, Spady DK, Dietschy JM. Saturated and unsaturated fatty acids independently regulate low density lipoprotein receptor activity and production rate. J Lipid Res. 1992;33(1):77-88. PMID: 1552235.
- Mensink RP, Zock PL, Kester ADM, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr. 2003;77(5):1146-55. PMID: 12716665.
- Hernaez A, Castaner O, Elosua R, Pinto X, Estruch R, Salas-Salvado J, et al. Mediterranean diet improves high-density lipoprotein function in high-cardiovascular-risk individuals: a randomized controlled trial. Circulation. 2017;135(7):633-43. PMID: 28193797.
- Delgado-Lista J, Alcala-Diaz JF, Torres-Pena JD, Quintana-Navarro GM, Fuentes F, Garcia-Rios A, et al.; CORDIOPREV Investigators. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomized controlled trial. Lancet. 2022;399(10338):1876-85. PMID: 35525255.
- Jimenez-Torres J, Alcala-Diaz JF, Torres-Pena JD, Gutierrez-Mariscal FM, Leon-Acuna A, Gomez-Luna P, et al. Mediterranean diet reduces atherosclerosis progression in coronary heart disease: an analysis of the CORDIOPREV randomised controlled trial. Stroke. 2021;52(8):2440-50. PMID: 34372670.
- Esposito K, Marfella R, Ciotola M, Di Palo C, Giugliano F, Giugliano G, et al. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: a randomized trial. JAMA. 2004;292(12):1440-6. PMID: 15383514.
- Gould KL, Ornish D, Scherwitz L, Brown S, Edens RP, Hess MJ, et al. Changes in myocardial perfusion abnormalities by positron emission tomography after long-term, intense risk factor modification. JAMA. 1995;274(11):894-901. PMID: 7674504.
- Satija A, Bhupathiraju SN, Spiegelman D, Chiuve SE, Manson JE, Willett W, et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J Am Coll Cardiol. 2017;70(4):411-22. PMID: 28728684.
- Dinu M, Pagliai G, Casini A, Sofi F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur J Clin Nutr. 2018;72(1):30-43. PMID: 28488692.
- Kahleova H, Levin S, Barnard ND. Cardio-metabolic benefits of plant-based diets. Nutrients. 2017;9(8):848. PMID: 28792455.
- Ros E, Nunez I, Perez-Heras A, Serra M, Gilabert R, Casals E, et al. A walnut diet improves endothelial function in hypercholesterolaemic subjects: a randomized crossover trial. Circulation. 2004;109(13):1609-14. PMID: 15037535.
- Henzel J, Kepka C, Kruk M, Wardziak L, Dzielinska Z, Ruzylllo W, et al. High-risk coronary plaque regression after intensive lifestyle intervention in nonobstructive coronary disease: a randomized study (DISCO-CT). JACC Cardiovasc Imaging. 2021;14(6):1192-202. PMID: 33341413.
- Esselstyn CB Jr. Defining an overdue requiem for palliative cardiovascular medicine. Am J Lifestyle Med. 2018;12(1):14-22. PMC6125067.