
 Q: Are endurance athletes really at higher risk for atrial fibrillation?
Q: Are endurance athletes really at higher risk for atrial fibrillation?
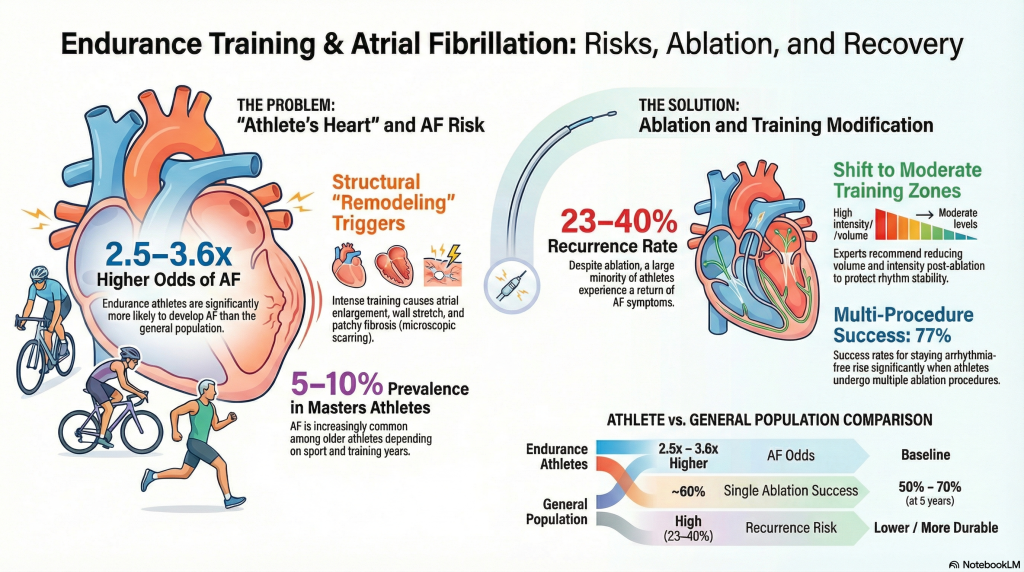
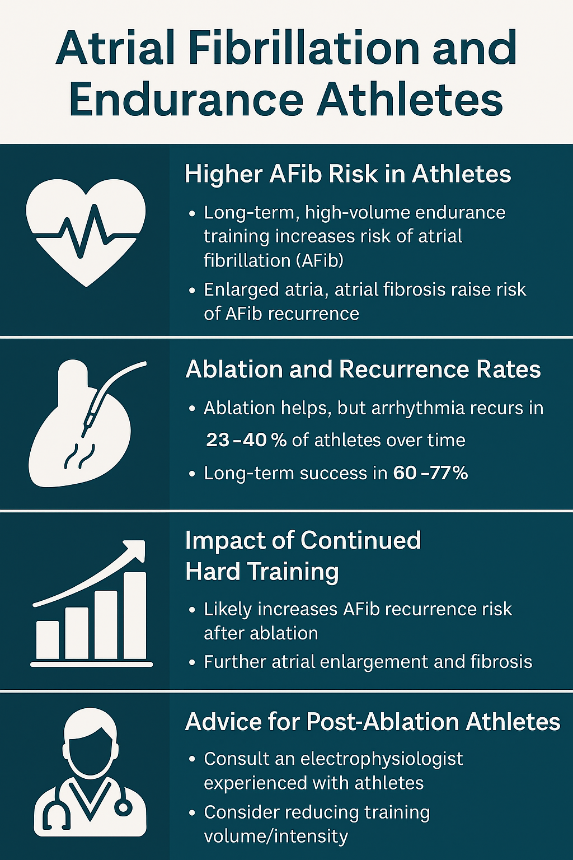
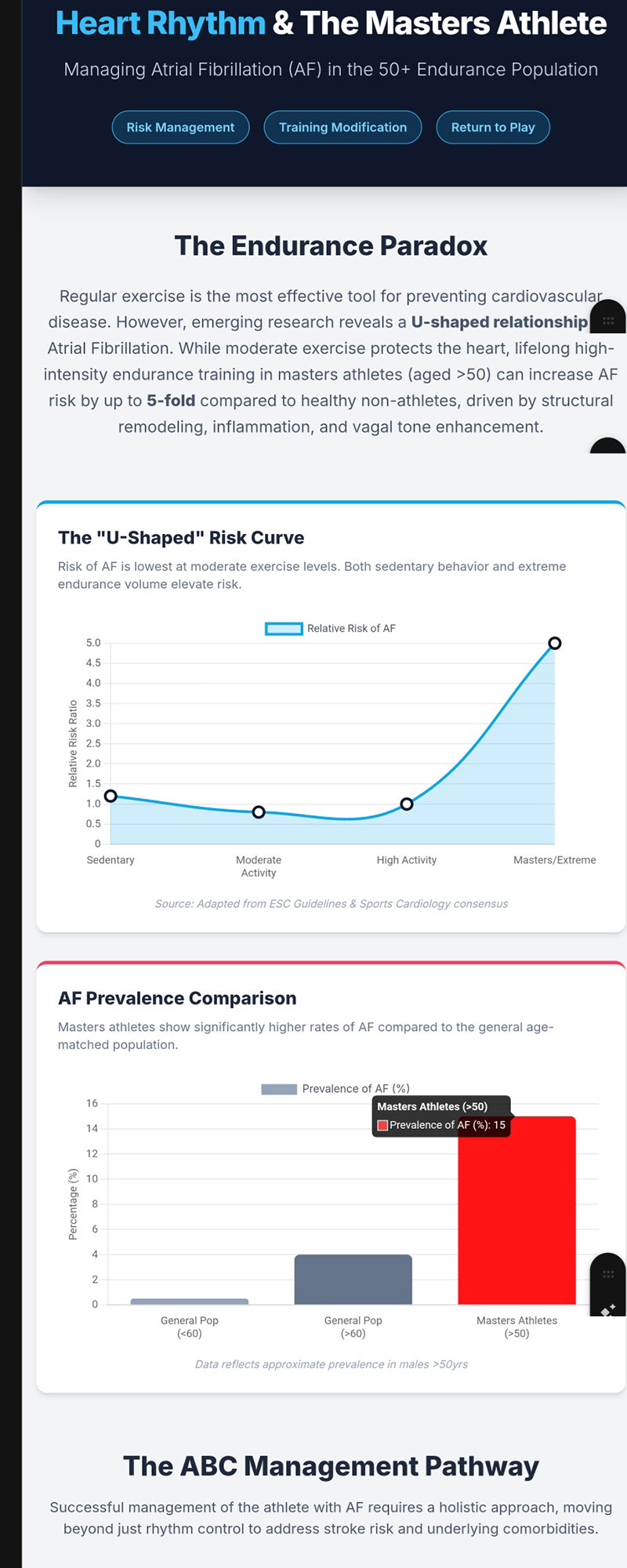
A: Yes. Atrial fibrillation (AF) is common in the general population, with a lifetime risk of roughly 1 in 4 adults.¹ While moderate exercise protects cardiovascular health, long-term, high-volume endurance training is associated with significantly higher AF rates. Meta-analyses show endurance athletes have about 2.5–3.6× higher odds of AF than non-athletes.² Among older Masters athletes, AF prevalence often reaches 5–10%, depending on the sport and cumulative years of training.³⁴
Q: What structural changes increase AF risk in highly trained athletes?
A: Years of intense endurance training can produce remodeling often called “athlete’s heart.” These changes include:
- Left atrial enlargement
- Atrial wall stretch from increased cardiac output
- Patchy fibrosis (microscopic scarring)
- Increased vagal tone, promoting electrical instability
Together, these changes create an arrhythmogenic substrate, making AF more likely both to develop and to recur.⁵ Structural studies also show that larger left atrial size from long-term endurance training is linked with a higher risk of incident AF.⁶
Q: After catheter ablation, what are the success and recurrence rates in endurance athletes?
A: Catheter ablation can substantially reduce AF burden, but recurrence is not rare.
- In endurance athletes, about 60% remain arrhythmia-free after a single ablation.⁷
- With multiple procedures, long-term success rises to around 77%.⁷
That means roughly 23–40% of endurance athletes experience recurrent AF despite modern ablation techniques.⁷
In the broader AF population, long-term studies report about 50–70% freedom from AF at five years, depending on whether patients have one or multiple procedures and on AF type.⁸⁹
Comparative work suggests that endurance athletes are less likely to remain arrhythmia-free two to three years after ablation than non-athletes treated with similar strategies.¹⁰
Q: Does continuing hard endurance training after ablation increase the chance of AF coming back?
A: The evidence strongly suggests yes, although current research cannot provide a precise percentage.
What we know:
- Long-term endurance athletes often have persistent atrial enlargement and fibrosis that do not fully reverse after ablation.⁵⁶
- Continued high-volume training maintains elevated atrial pressures, stretch, and wall stress, the same forces that contributed to AF in the first place.⁵⁶
- Atrial enlargement and fibrosis are well-established predictors of AF recurrence after ablation.⁵
- Ablation outcome studies show substantial recurrence rates in endurance athletes and generally less durable rhythm control compared with non-athletes.⁷¹⁰
What is not yet known: no published long-term prospective study has directly compared post-ablation athletes who continue high-intensity endurance training versus those who reduce it. As a result, we cannot state an exact “X% increase” in relapse risk — but mechanistically and clinically, ongoing hard training almost certainly raises the probability of AF coming back.
Q: Why don’t we have exact numbers on relapse risk from continued high-intensity training?
A: To get exact numbers, researchers would need to follow two groups of post-ablation endurance athletes over many years: one group continuing high-intensity training, the other reducing it, with careful tracking of AF recurrence. Such a trial has been proposed, but results are not yet available. Until then, recommendations are based on physiology, imaging data, and observed ablation outcomes in athletes.²⁵⁶⁷
Q: What do electrophysiologists generally recommend for athletes after ablation?
Most experts advise reducing training intensity and/or volume, at least temporarily, especially for athletes who:
- Have left atrial enlargement
- Show atrial fibrosis on imaging
- Have recurrent or persistent AF
- Are older Masters athletes
- Train year-round at high volume or intensity
This does not mean stopping exercise altogether. Rather, it usually means shifting toward moderate, sustainable training zones and avoiding chronic extreme endurance loads while rhythm stability and atrial size are monitored.⁵⁶
Q: Can an endurance athlete return to high-level training after ablation?
A: Some can, particularly those with paroxysmal AF, relatively small atria, and minimal fibrosis. Many athletes feel dramatically better after ablation.
However, several realities remain:
- The arrhythmogenic substrate (enlarged and sometimes fibrotic atria) often persists.⁵⁶
- Even with good treatment, 23–40% of endurance athletes will have AF recur over time.⁷
- Continued extreme endurance training likely increases the probability of recurrence, even though we cannot yet quantify by how much.⁷¹⁰
A sports cardiologist or electrophysiologist familiar with athletes is best positioned to help balance performance goals with long-term heart health.
Q: What’s the bottom line?
- Endurance athletes have a higher baseline AF risk than non-athletes.²³⁴
- Catheter ablation reduces symptoms and AF burden but is not guaranteed to be curative.⁷⁸⁹
- Continued high-intensity endurance training likely raises AF recurrence risk by maintaining atrial stretch and structural remodeling.⁵⁶⁷¹⁰
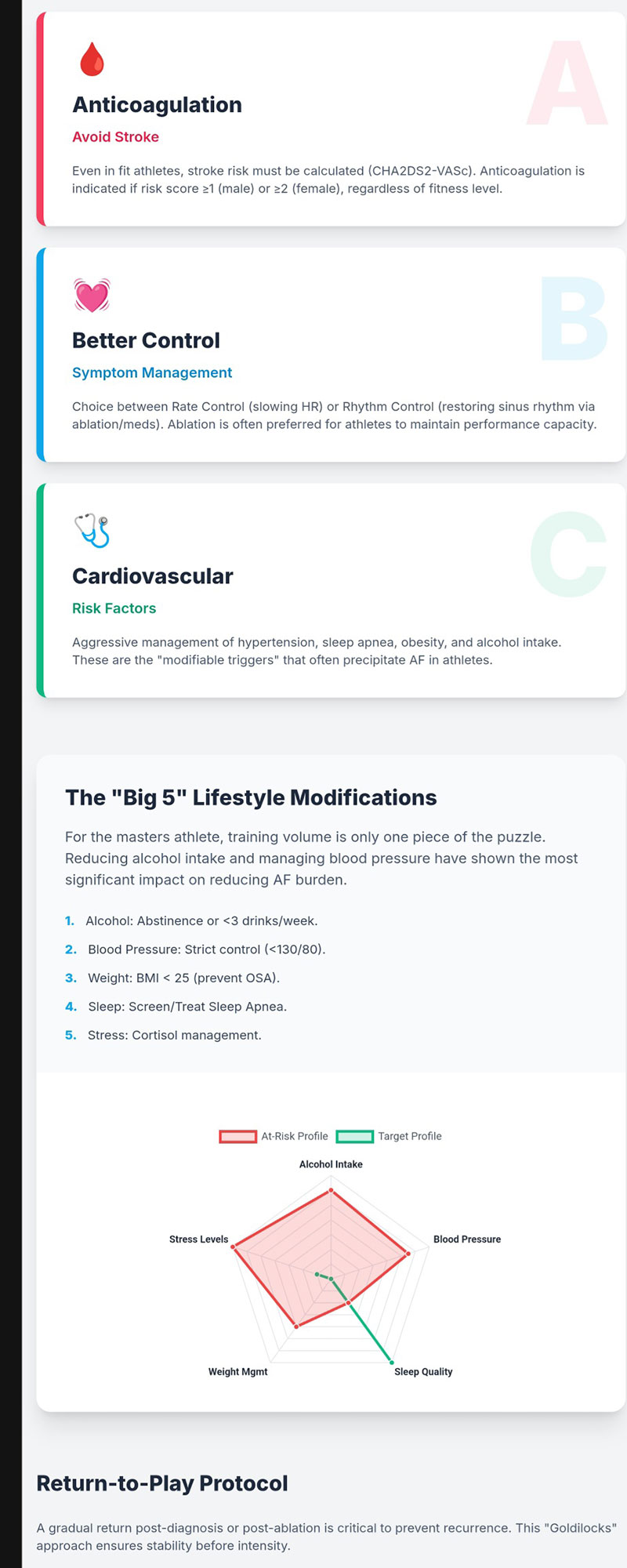
- Moderating training load and aggressively managing other risk factors (blood pressure, weight, sleep apnea, alcohol, etc.) may help improve long-term rhythm stability.⁵⁶
- Individualized care from a knowledgeable electrophysiologist is essential for any athlete navigating AF and ablation.
References
- Heeringa J, van der Kuip DA, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J. 2006;27(8):949-953. doi:10.1093/eurheartj/ehi825
- Abdulla J, Nielsen JR. Is the risk of atrial fibrillation higher in athletes than in the general population? A systematic review and meta-analysis. Europace. 2009;11(9):1156-1159. doi:10.1093/europace/eup197
- Calvo N, Brugada J, Sitges M, Mont L. Atrial fibrillation and atrial flutter in athletes. Br J Sports Med. 2012;46 Suppl 1:i37-i43. doi:10.1136/bjsports-2012-091171
- Newman W, Parry-Williams G, Wiles J, et al. Risk of atrial fibrillation in athletes: a systematic review and meta-analysis. Br J Sports Med. 2021;55(21):1233-1238. doi:10.1136/bjsports-2021-103994
- Elliott AD, Maatman B, Emery MS, Sanders P. The role of exercise in atrial fibrillation prevention and promotion: Finding optimal ranges for health. Heart Rhythm. 2017;14(11):1713-1720. doi:10.1016/j.hrthm.2017.07.001
- Heitmann KA, Løchen ML, Stylidis M, Hopstock LA, Schirmer H, Morseth B. Associations between physical activity, left atrial size and incident atrial fibrillation: the Tromsø Study 1994-2016. Open Heart. 2022;9(1):e001823. doi:10.1136/openhrt-2021-001823
- Mandsager KT, Phelan DM, Diab M, et al. Outcomes of Pulmonary Vein Isolation in Athletes. JACC Clin Electrophysiol. 2020;6(10):1265-1274. doi:10.1016/j.jacep.2020.05.009
- Ngo L, Lee XW, Elwashahy M, et al. Freedom from atrial arrhythmia and other clinical outcomes at 5 years and beyond after catheter ablation of atrial fibrillation: a systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2023;9(5):447-458. doi:10.1093/ehjqcco/qcad037
- Ichijo S, Miyazaki S, Kusa S, et al. Impact of catheter ablation of atrial fibrillation on long-term clinical outcomes in patients with heart failure. J Cardiol. 2018;72(3):240-246. doi:10.1016/j.jjcc.2018.02.012
- Carbone A, Monda E, Ferrara F, et al. Aortic Dimension in Elite Athletes: Updated Systematic Review and Meta-Analysis. Eur J Prev Cardiol. Published online November 26, 2024. doi:10.1093/eurjpc/zwae385