
Clinical Paradigms of Disease Resolution: Biological Differentiation between the Cure of Pathological Processes and the Reversal of Structural Damage
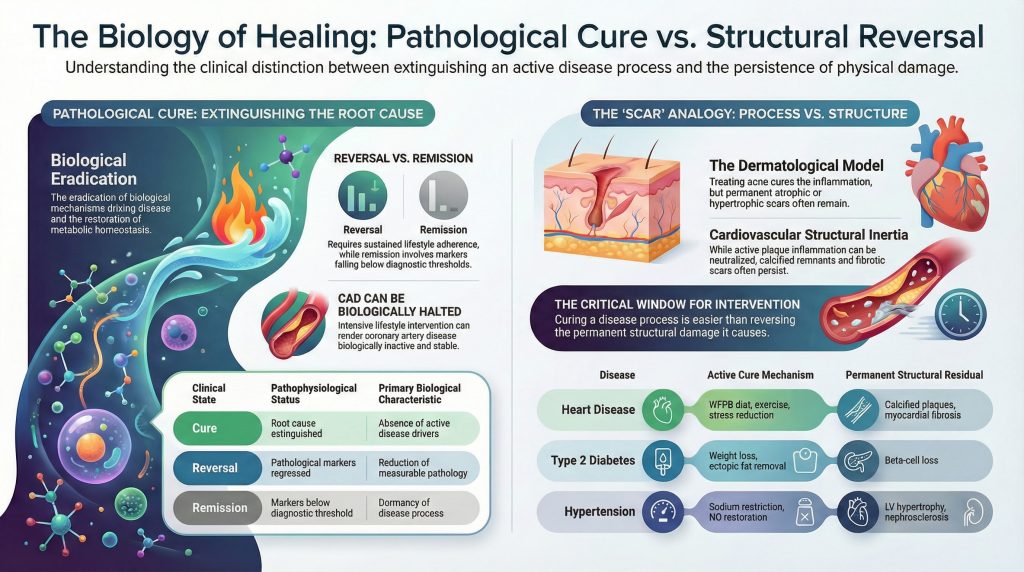
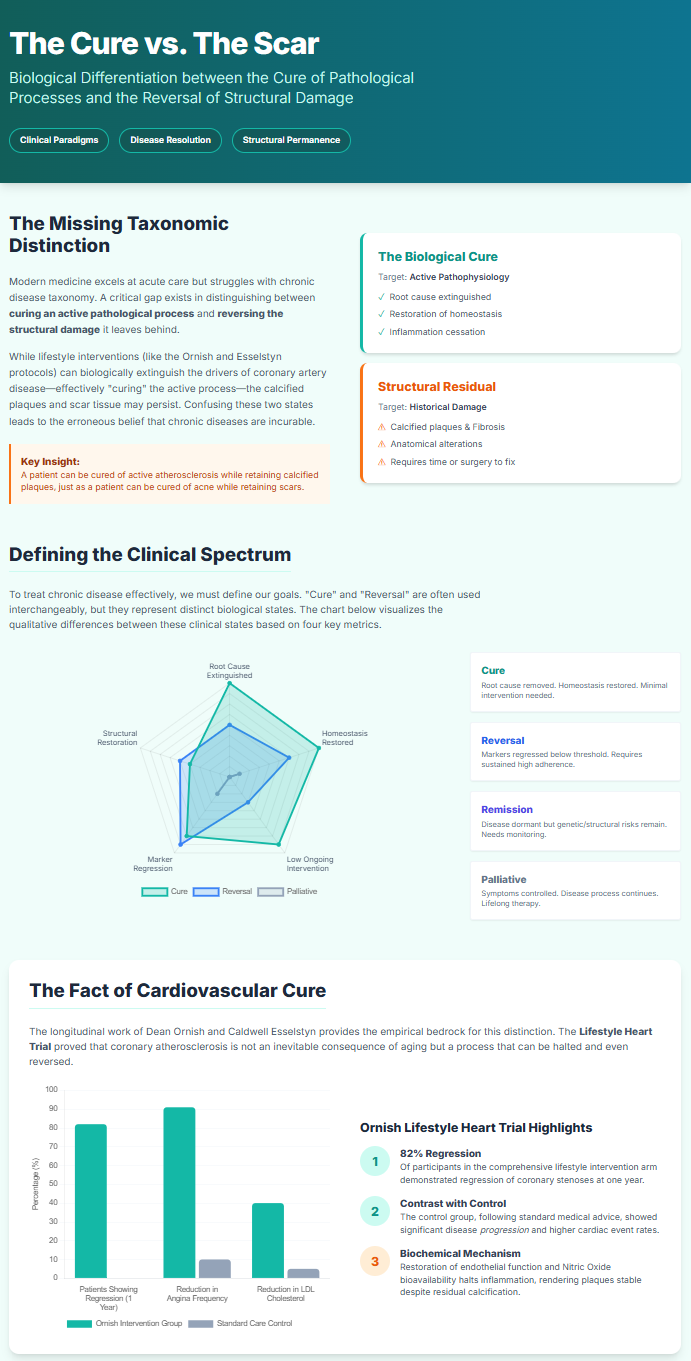
The medical community has historically distinguished between the resolution of acute illness and the long-term management of chronic disease. As lifestyle medicine has matured into a formal clinical discipline, it has exposed a critical gap in medical taxonomy: the failure to clearly differentiate between the cure of an active pathological process and the reversal of structural damage produced by that process. Within dominant clinical paradigms, most chronic diseases are treated through symptom control, risk reduction, and delay of complications rather than through eradication of underlying biological drivers.¹ Nevertheless, a growing body of empirical evidence—most prominently from the longitudinal work of Dean Ornish and Caldwell Esselstyn—demonstrates that coronary artery disease (CAD), the leading cause of global mortality, can have its active disease process halted and rendered biologically inactive through intensive lifestyle intervention.² This state constitutes a cure at the level of pathophysiology, even though it does not invariably result in complete restoration of normal vascular anatomy or elimination of pre‑existing structural injury.⁵
The conceptual challenge of distinguishing cure from reversal is well illustrated by the dermatological example of severe acne vulgaris. In acne, the disease process consists of inflammation driven by follicular hyperkeratinization, excess sebum production, and microbial proliferation.⁷ When treated effectively, this process can be cured, resulting in the cessation of new lesions. Yet many patients are left with permanent atrophic or hypertrophic scars—structural alterations of the skin that no longer represent active disease.¹⁰ This distinction provides a clinically useful framework for cardiovascular medicine: a patient may be cured of active atherosclerosis and rendered highly resistant to acute coronary events while still retaining calcified plaques or ischemic limitations that represent historical damage rather than ongoing disease activity.⁶
Taxonomic Definitions in Chronic Disease Management
To navigate chronic disease resolution with precision, clinicians must distinguish the status of the pathological process from the condition of the affected organ’s structure. A cure denotes eradication of the biological mechanisms driving disease and restoration of metabolic homeostasis, such that continued clinical intervention is minimal or unnecessary.¹⁵ Reversal, in contrast, refers to regression of measurable disease markers—such as hyperglycemia or arterial stenosis—below diagnostic thresholds, typically requiring sustained behavioral adherence to prevent recurrence.³
Clinical State | Pathophysiological Status | Required Intervention Post‑Resolution | Primary Biological Characteristic | Cure | Root cause extinguished; homeostasis restored | Minimal to none | Absence of active disease drivers | Reversal | Pathological markers regressed | Sustained lifestyle adherence | Reduction of measurable pathology | Remission | Markers below diagnostic threshold | Continuous monitoring | Dormancy of disease process | Palliative | Symptoms controlled; cause persists | Lifelong therapy | Suppression without resolution
This distinction is particularly relevant in type 2 diabetes mellitus (T2D). Remission is defined as an A1C below 6.5% for at least three months without pharmacologic therapy, yet the condition is rarely labeled a cure because genetic susceptibility and residual beta‑cell dysfunction persist.¹⁵ Environmental stressors, such as weight regain, can reactivate the disease process.¹⁷ Similarly, in CAD, patients may achieve biological stability in which plaque inflammation and rupture risk are neutralized, even though calcified or fibrotic remnants of prior disease remain.⁶
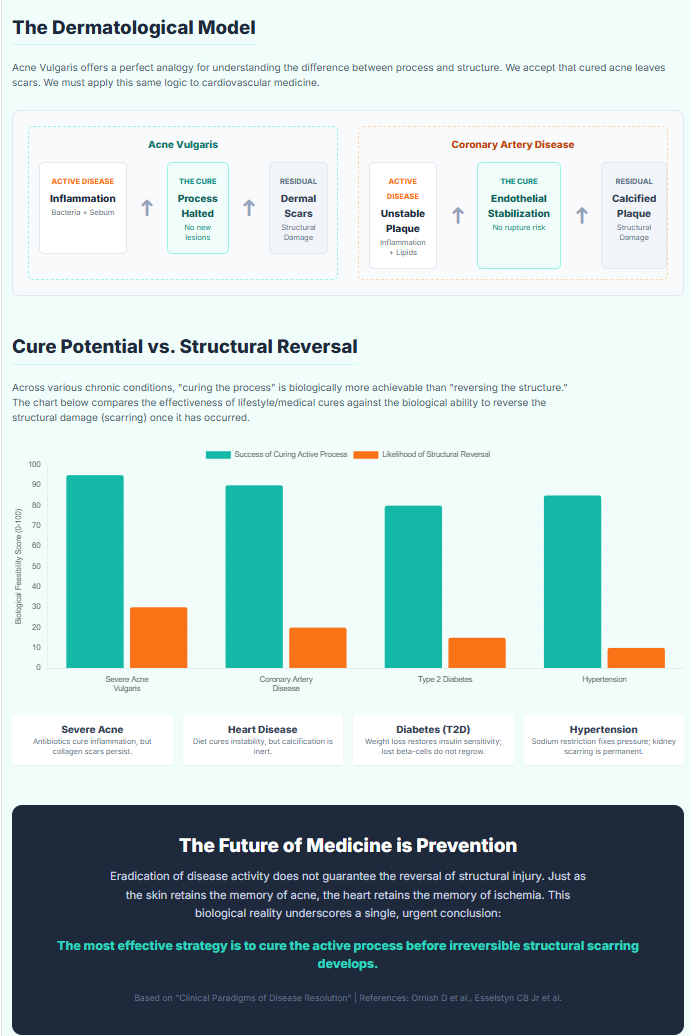
The Dermatological Model: Curing the Process versus Reversing the Scar
The analogy between acne and atherosclerosis is not merely metaphorical; it reflects shared mechanisms of inflammation‑driven tissue remodeling. Acne targets the pilosebaceous unit, where Cutibacterium acnes initiates immune cascades that may culminate in follicular rupture and dermal injury.⁹ When treated with retinoids, antibiotics, or hormonal modulation, the cure is defined by elimination of inflammatory triggers and normalization of keratinization.⁷
Despite resolution of the active inflammatory process, structural sequelae often remain. These scars are classified by collagen dynamics:
Atrophic scars (ice‑pick, boxcar, rolling) result from collagen loss and dermal matrix destruction during intense inflammation.⁸
Hypertrophic scars and keloids reflect excessive collagen deposition, sometimes extending beyond the original lesion.⁸
These residual structural changes may exert lasting psychological and functional effects long after the disease itself has been cured.¹² Analogously, individuals with stabilized CAD may retain fixed stenoses or myocardial scars that impair perfusion despite elimination of unstable plaque biology.⁵ Thus, curing an inflammatory disease process is biologically more achievable than reversing the structural damage it leaves behind.
The Fact of Cardiovascular Cure: Ornish and Esselstyn Paradigms
Contrary to the belief that CAD is an inevitable consequence of aging, extensive clinical research demonstrates that atherosclerosis is largely a lifestyle‑mediated condition whose active progression can be halted.¹³ This conclusion is supported by decades of peer‑reviewed investigation.
The Ornish Lifestyle Heart Trial
Dean Ornish provided early definitive evidence that coronary atherosclerosis progression could be stopped and modestly reversed without lipid‑lowering drugs.² Using quantitative coronary arteriography and positron emission tomography, the Lifestyle Heart Trial evaluated the effects of a comprehensive intervention including a low‑fat, whole‑food, plant‑based diet, moderate exercise, stress management, and social support.² Eighty‑two percent of participants in the intervention arm demonstrated regression of coronary stenoses at one year.² At five years, this group exhibited further regression and significantly fewer cardiac events than controls receiving standard dietary advice.²
The Esselstyn Protocol and Endothelial Stabilization
Caldwell Esselstyn’s work emphasized nutritional primacy in restoring endothelial function.⁴ By eliminating animal products and added oils, his protocol aims to normalize nitric oxide bioavailability and suppress endothelial inflammation.¹³ Long‑term observational cohorts of adherent patients with advanced CAD demonstrated near‑complete cessation of major cardiac events.¹⁴ Esselstyn proposes that sustained LDL levels below 70 mg/dL combined with preserved endothelial nitric oxide signaling effectively extinguish the active disease process.¹³
Biological Mechanisms Underlying Disease Extinction
Lifestyle‑mediated disease resolution reflects coordinated biochemical shifts rather than isolated pharmacologic effects. Endothelial nitric oxide restoration improves vasodilation, inhibits leukocyte adhesion, and reduces thrombogenicity.¹³ High‑fat meals acutely impair endothelial function, whereas nitrate‑rich plant foods enhance nitric oxide bioavailability.¹³
Trimethylamine N‑oxide (TMAO) has emerged as a diet‑associated biomarker linked to increased cardiovascular risk. TMAO production depends on gut microbial metabolism of carnitine and choline, primarily derived from animal products. Individuals adhering to strict plant‑based diets demonstrate markedly reduced TMAO generation, contributing to risk attenuation.
Why Disease Cure Outpaces Structural Reversal
While inflammatory atherogenesis responds rapidly to metabolic normalization, structural damage exhibits biological inertia. Plaque calcification represents a regulated, osteogenic‑like process mediated by vascular smooth muscle cell differentiation.⁵ Early lipid‑rich plaques are more amenable to regression, whereas mature calcified lesions often persist despite disease quiescence.¹⁸ Genomic studies demonstrate that early and advanced plaques are governed by distinct regulatory networks, limiting reversibility in late‑stage disease.
Myocardial infarction further illustrates this principle: necrotic myocardium is replaced by fibrotic scar tissue incapable of contractile recovery. Lifestyle intervention can prevent subsequent infarction but cannot readily regenerate lost myocardium, leading to chronic ischemic limitations.
Residual Cardiovascular Risk
Residual cardiovascular risk refers to adverse events occurring despite optimal suppression of active disease.⁶ Contributors include persistent calcification, arterial stiffness, incomplete plaque stabilization, and low‑grade inflammation.⁶ These risks are structural rather than process‑driven and parallel scarring phenomena observed across chronic disease models.
Comparative Disease Models
This cure‑versus‑scar dichotomy recurs throughout medicine. In T2D, removal of ectopic fat restores insulin sensitivity, yet prolonged disease may result in irreversible beta‑cell loss.³ In hypertension, blood pressure normalization may not reverse left ventricular hypertrophy or nephrosclerosis once structural remodeling has occurred.
Clinical States and Biological Resolution Framework
| Clinical State | Pathophysiological Status | Primary Biological Characteristic | Required Intervention Post-Resolution |
| Cure | Root cause extinguished; homeostasis restored | Absence of active disease drivers | Minimal to none |
| Reversal | Pathological markers regressed | Reduction of measurable pathology | Sustained lifestyle adherence |
| Remission | Markers below diagnostic threshold | Dormancy of disease process | Continuous monitoring |
| Palliative | Symptoms controlled; cause persists | Suppression without resolution | Lifelong therapy |
Conclusion
Coronary artery disease can have its active pathological process extinguished through intensive lifestyle intervention.² However, eradication of disease activity does not guarantee reversal of structural injury. As with cured acne leaving dermal scars, the stabilized heart may retain calcified or ischemic remnants of prior disease.⁵ This reality underscores the urgency of early intervention: the most effective strategy is to cure the process before irreversible scarring develops.¹⁸ The future of medicine lies not in managing inevitable decline, but in applying proven biological cures early enough to prevent permanent damage from forming.
References
- Pizzorno J. Can We Say “Cure”?. Integr Med (Encinitas). 2016;15(5):8-12.
- Ornish D, Brown SE, Scherwitz LW, et al. Can lifestyle changes reverse coronary heart disease? The Lifestyle Heart Trial. Lancet. 1990;336(8708):129-133. doi:10.1016/0140-6736(90)91656-u
- Taylor R, Al-Mrabeh A, Sattar N. Understanding the mechanisms of reversal of type 2 diabetes. Lancet Diabetes Endocrinol. 2019;7(9):726-736. doi:10.1016/S2213-8587(19)30076-2
- Esselstyn CB Jr, Gendy G, Doyle J, Golubic M, Roizen MF. A way to reverse CAD?. J Fam Pract. 2014;63(7):356-364b.
- Isoda K, Nishikawa K, Kamezawa Y, et al. Osteopontin plays an important role in the development of medial thickening and neointimal formation. Circ Res. 2002;91(1):77-82. doi:10.1161/01.res.0000025268.10302.0c
- Ciccarelli G, Conte S, Cimmino G, Maiorano P, Morrione A, Giordano A. Mitochondrial Dysfunction: The Hidden Player in the Pathogenesis of Atherosclerosis?. Int J Mol Sci. 2023;24(2):1086. Published 2023 Jan 6. doi:10.3390/ijms24021086
- Connolly D, Vu HL, Mariwalla K, Saedi N. Acne Scarring-Pathogenesis, Evaluation, and Treatment Options. J Clin Aesthet Dermatol. 2017;10(9):12-23.
- Fabbrocini G, Annunziata MC, D’Arco V, et al. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893080. doi:10.1155/2010/893080
- Zhou L, Liu X, Li X, He X, Xiong X, Lai J. Epidermal Barrier Integrity is Associated with Both Skin Microbiome Diversity and Composition in Patients with Acne Vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2065-2075. Published 2022 Sep 28. doi:10.2147/CCID.S377759
- DermNet NZ. Acne scarring. https://dermnetnz.org.
- Ryguła I, Pikiewicz W, Kaminiów K. Impact of Diet and Nutrition in Patients with Acne Vulgaris. Nutrients. 2024;16(10):1476. Published 2024 May 14. doi:10.3390/nu16101476
- Esselstyn CB Jr. Resolving the Coronary Artery Disease Epidemic Through Plant-Based Nutrition. Prev Cardiol. 2001;4(4):171-177. doi:10.1111/j.1520-037x.2001.00538.x
- Delgado-Lista J, Alcala-Diaz JF, Torres-Peña JD, et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. Lancet. 2022;399(10338):1876-1885. doi:10.1016/S0140-6736(22)00122-2
- Aminian A, Brethauer SA, Andalib A, et al. Can Sleeve Gastrectomy “Cure” Diabetes? Long-term Metabolic Effects of Sleeve Gastrectomy in Patients With Type 2 Diabetes. Ann Surg. 2016;264(4):674-681. doi:10.1097/SLA.0000000000001857
- Taylor R, Al-Mrabeh A, Sattar N. Understanding the mechanisms of reversal of type 2 diabetes. Lancet Diabetes Endocrinol. 2019;7(9):726-736. doi:10.1016/S2213-8587(19)30076-2
- Zhu D, Mackenzie NC, Farquharson C, Macrae VE. Mechanisms and clinical consequences of vascular calcification. Front Endocrinol (Lausanne). 2012;3:95. Published 2012 Aug 6. doi:10.3389/fendo.2012.00095
- Thomas MS, Fernandez ML. Trimethylamine N-Oxide (TMAO), Diet and Cardiovascular Disease. Curr Atheroscler Rep. 2021;23(4):12. Published 2021 Feb 17. doi:10.1007/s11883-021-00910-x
- Arora S, Matsushita K, Qamar A, Stacey RB, Caughey MC. Early versus late percutaneous revascularization in patients hospitalized with non ST-segment elevation myocardial infarction: The atherosclerosis risk in communities surveillance study. Catheter Cardiovasc Interv. 2018;91(2):253-259. doi:10.1002/ccd.27156
- Sutton MG, Sharpe N. Left ventricular remodeling after myocardial infarction: pathophysiology and therapy. Circulation. 2000;101(25):2981-2988. doi:10.1161/01.cir.101.25.2981
- Liga R, Colli A, Taggart DP, Boden WE, De Caterina R. Myocardial Revascularization in Patients With Ischemic Cardiomyopathy: For Whom and How. J Am Heart Assoc. 2023;12(6):e026943. doi:10.1161/JAHA.122.026943
- Bidani AK, Griffin KA. Pathophysiology of hypertensive renal damage: implications for therapy. Hypertension. 2004;44(5):595-601. doi:10.1161/01.HYP.0000145180.38707.84